
 Fodi Kyriakos explores how the COVID-19 pandemic could be the catalyst for change in radiology and encourages our community to grasp the opportunity to “seize the moment” and plan for recovery.
Fodi Kyriakos explores how the COVID-19 pandemic could be the catalyst for change in radiology and encourages our community to grasp the opportunity to “seize the moment” and plan for recovery.
At the beginning of 2020, if someone had told radiology leaders that all NHS outstanding reporting backlogs would be reduced to virtually zero by May, I’m sure they would have looked at you in disbelief and asked what sorcery had been involved, but this situation is exactly where we find ourselves today.
Normalcy Bias – Noun [edit]
normalcy bias (plural normalcy biases)
The phenomenon of disbelieving one’s situation when faced with grave and imminent danger and/or catastrophe. As in over focusing on the actual phenomenon instead of taking evasive action, a state of paralysis.
Historical challenges
In the past, it has often taken lots of effort to either invoke or accept change of any kind in radiology and for those managing services, there’s also been a certain amount of risk associated with putting your head above the parapet or being a trailblazer. It has been sometimes easier to follow the well-trodden path rather than to create a new one. Workloads and budgetary constraints have also been a disabler, restricting decision making to the ‘here and now’. This has resulted in failing, or in most cases, not being able to foresee or plan for events that have never happened before, such as an event like a pandemic crisis. Psychology refers to this state of being as normalcy bias. For those who are not familiar with the term, you will certainly be aware of its connotations and radiology now finds itself at this cross-roads.
Ever since the introduction of digital radiography and PACS, NHS radiology reporting backlogs have been a contentious issue among experts, and a recurring feature in the mainstream media! Often being highlighted (and with some justification) in relation to areas such as missed cancer diagnosis, where even the slightest of delays can have a significant bearing on the overall outcome.
Serious backlogs
The extent to which backlogs were a serious issue in the UK was further exacerbated by various Care Quality Commission (CQC) inspections, which raised concerns regarding reporting backlogs that resulted in delayed or missed diagnosis of conditions that may have otherwise been picked up.
By the end of February 2020, the situation of backlogs was as much an issue as at any time before. Insufficient reporting capacity had led to a build-up of outstanding reports, which in turn meant that outsourcing was at its highest ever levels and growing pressures to meet new deadlines, such as the cancer pathway targets, were increasingly exposing the lack of options available to resolve the problem.
So, you would have been excused if you thought that a crisis such as the COVID-19 pandemic would simply exacerbate the reporting challenges facing radiology. However, this has not been the case. Instead, we have witnessed radiology’s own “clear the decks” exercise, where in fact the complete opposite situation has occurred, resulting in backlogs across the UK being virtually eliminated. Who would have thought that the worst crisis to hit the country (and the world) in 75 years would be a catalyst for NHS radiology departments to press the reset button?

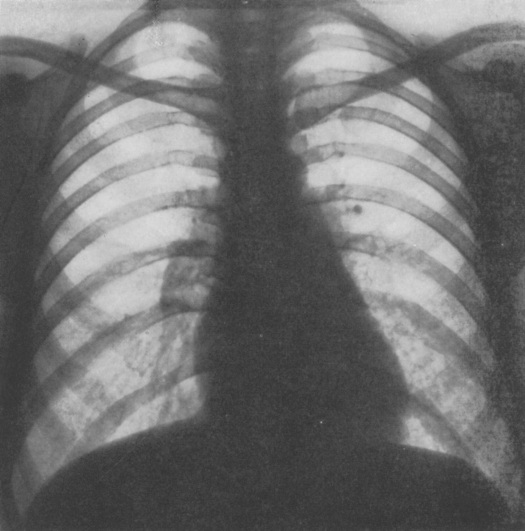
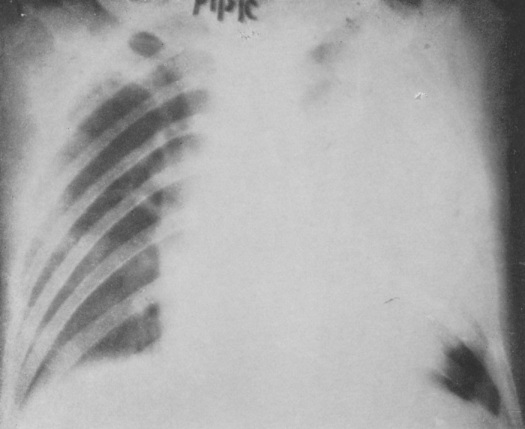
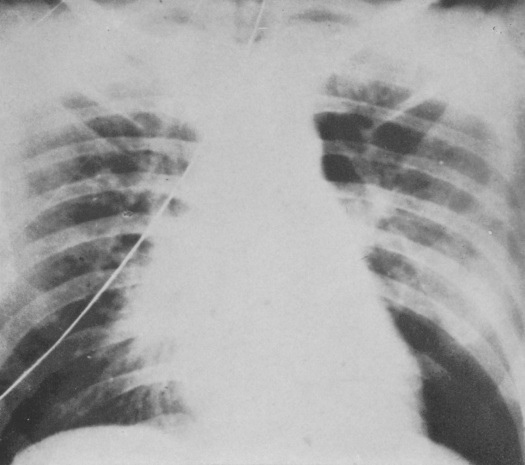
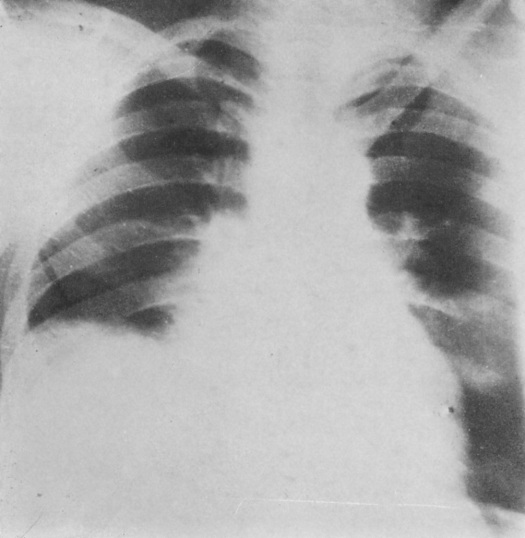
Of course, we recognise the superficial nature of this situation. During the pandemic, practically all routine referral activity came to a grinding halt, which allowed radiology to concentrate on COVID-19 and Emergency Department (ED) patients. Chest X-rays and CTs were identified as two of the key diagnostic tools for the virus, but the volumes were manageable. Accident and Emergency footfall was reduced to almost 50% of its usual figures, so reporters were practically able to deliver a ‘Hot-Reporting’ examination for every patient requiring imaging. Something which ED and Intensive care unit (ICU) consultants have grown quickly accustomed to.
During this time, radiology was also still required to work to critical staffing levels, so radiographers and radiologists were covering 24/7 rotas, but due to the lack of activity outside of portable X-ray scanning in ICU, many staff were not being utilised. So, while this enabled the catch up in radiology reporting to take place, what we witnessed was the ‘ying and yang’ of radiology. On the one hand, integral to the continuity of a patient’s pathway and critical to defining an outcome – AND on the other hand, completely dependent on throughput from referrers to maintain activity levels.
Seizing the moment!
So what happens next? Well, in a world where we can guarantee almost nothing, in this situation, we can guarantee that radiology will remain the centre point for the recovery phase of the pandemic, but with the added challenge of complying to ‘social distancing’ and ‘equipment cleaning’ guidelines, how do we manage the continuation of treating COVID-19 patients, while reintroducing ‘business as usual’ and ‘deferred’ patients whose treatment has been delayed?
The “Reset Button” has enabled something else to happen. For the first time, there is now some headspace to plan for the recovery phase and for the next phase at least, there is now funding available to support the recovery. So how do we avoid going back to where we were before the pandemic? How do we seize the moment?
Time to make the changes!
Albert Einstein once famously said: “We can’t solve problems by using the same kind of thinking we used when we created them.” This quote has never been more poignant in the present day and while the pressure to manage change will be at its highest, this is the right time to make these changes happen! With the benefit of ‘The Reset Button’, if we can learn from the past and apply new ways of working moving forward, we can avoid falling into the trap of the normalcy bias and witness the radiology reset button offering a new, efficient and more streamlined radiology department moving forward.
Everything you wanted to know about radiology but were afraid to ask…
On Wednesday 17 June, a live event organised by InHealth, in partnership with The British Institute of Radiology and the Society of Radiographers is taking place, titled: “The Radiology reset button has been pressed”. The aim is to tackle these challenges and support radiology managers as they enter the recovery phase. It will bring together senior figures from radiology and within healthcare to offer insights, opinions and advice on how we can approach this coming period and use what positives we have experienced during the pandemic to create service improvements throughout radiology.
There will be opportunities for radiology managers, clinical leads, radiographers and radiologists to put their questions to the speakers in the panel discussions after their presentations.
REGISTER FOR THE RADIOLOGY RESET BUTTON HAS BEEN PRESSED HERE
(The event is free for all)
About Fodi Kyriakos
Mr Fodi Kyriakos is a former director of RIG Healthcare and founder of RIG Reporting,
the UK’s first provider of external radiographer reporting services. In 2016 he joined The InHealth Group following its acquisition of RIG Reporting and is now the Head of Reporting across the Group. His service specialises in delivering plain film reporting solutions and is the only provider to offer both on-site and telereporting services.
Fodi has over 22 years experience in workforce and staffing solutions and 17 years working exclusive within Imaging and Oncology. He is a member of the Institute of Healthcare Managers and a regular contributor of professional development events across radiology.













 This was a time when, in this Cinderella of specialties, physics planning was achieved by the superposition of two dimensional radiation plots (isodoses) ,using tracing paper and pencils, to produce summated maps of the distribution. The crude patient outlines were derived from laborious isocentric distance measurements augmented by the essential “flexicurve”. The whole planning process was slow and labour intensive fraught with errors and ridiculed by colleagues in the perceived prestigious scientific and clinical disciplines. The principal platform for external beam radiotherapy delivery, the Linear Accelerator (LinAc), had also reached something of a plateau of development, albeit with improved reliability, but few fundamental changes. Caesium tubes were transported from the “radium safe”, locked in an underground vault, to the operating theatre in a lead-lined trolley, where they were only loaded into “central tubes” and “ovoids” after the examination under anaesthetic (which was performed with the patient in the knee-chest position); they were then manually placed into the patient, who went to be nursed on an open ward, albeit behind strategically placed lead barriers.
This was a time when, in this Cinderella of specialties, physics planning was achieved by the superposition of two dimensional radiation plots (isodoses) ,using tracing paper and pencils, to produce summated maps of the distribution. The crude patient outlines were derived from laborious isocentric distance measurements augmented by the essential “flexicurve”. The whole planning process was slow and labour intensive fraught with errors and ridiculed by colleagues in the perceived prestigious scientific and clinical disciplines. The principal platform for external beam radiotherapy delivery, the Linear Accelerator (LinAc), had also reached something of a plateau of development, albeit with improved reliability, but few fundamental changes. Caesium tubes were transported from the “radium safe”, locked in an underground vault, to the operating theatre in a lead-lined trolley, where they were only loaded into “central tubes” and “ovoids” after the examination under anaesthetic (which was performed with the patient in the knee-chest position); they were then manually placed into the patient, who went to be nursed on an open ward, albeit behind strategically placed lead barriers. In the latter half of the eighties these solutions began to crystallise. Computers were being introduced across the NHS and their impact was not lost in radiotherapy. Pads of tracing paper were replaced with the first generation of planning computers. The simple “Bentley-Milan” algorithms could account for patient outlines accurately and speedily and optimising different beam configurations became practical. Consideration of Organs at Risk, as defined by the various International Commission on Radiation Units (ICRU) publications, became increasingly relevant. Recognition of the importance of delineating the target volumes and protecting normal tissue required improved imaging and this was provided by the new generation of CT scanners. In the nineties these were shared facilities with diagnostic radiology departments. However, the improvements provided by this imaging, enabling accurate 3-dimensional mapping of the disease with adjacent normal tissues and organs at risk, dictated their inclusion into every radiotherapy department soon after the millennium. The added bonus of using the grey scale pixel information, or Hounsfield numbers, to calculate accurate radiation transport distributions soon followed when the mathematical and computer technology caught up with the task. The value of MR and Positron Emission Tomography (PET) imaging was also recognised in the diagnosis, staging and planning of radiotherapy and the new century saw all of these new technologies embedded within the department.
In the latter half of the eighties these solutions began to crystallise. Computers were being introduced across the NHS and their impact was not lost in radiotherapy. Pads of tracing paper were replaced with the first generation of planning computers. The simple “Bentley-Milan” algorithms could account for patient outlines accurately and speedily and optimising different beam configurations became practical. Consideration of Organs at Risk, as defined by the various International Commission on Radiation Units (ICRU) publications, became increasingly relevant. Recognition of the importance of delineating the target volumes and protecting normal tissue required improved imaging and this was provided by the new generation of CT scanners. In the nineties these were shared facilities with diagnostic radiology departments. However, the improvements provided by this imaging, enabling accurate 3-dimensional mapping of the disease with adjacent normal tissues and organs at risk, dictated their inclusion into every radiotherapy department soon after the millennium. The added bonus of using the grey scale pixel information, or Hounsfield numbers, to calculate accurate radiation transport distributions soon followed when the mathematical and computer technology caught up with the task. The value of MR and Positron Emission Tomography (PET) imaging was also recognised in the diagnosis, staging and planning of radiotherapy and the new century saw all of these new technologies embedded within the department. LinAc technology also received added impetus. Computers were firstly coupled as a front end to conventional LinAcs as a safety interface to reduce the potential for “pilot error”. Their values were soon recognised by the manufacturers and were increasingly integrated into the machine, monitoring performance digitally and driving the new developments of Multi Leaf Collimators (MLC) and On Board Imaging (OBI).
LinAc technology also received added impetus. Computers were firstly coupled as a front end to conventional LinAcs as a safety interface to reduce the potential for “pilot error”. Their values were soon recognised by the manufacturers and were increasingly integrated into the machine, monitoring performance digitally and driving the new developments of Multi Leaf Collimators (MLC) and On Board Imaging (OBI). Dr David A L Morgan began training in Radiotherapy & Oncology as a Registrar in 1977, and in 1982 was appointed a Consultant in the specialty in Nottingham, continuing to work there until his retirement in 2011. He joined the BIR in 1980 and at times served as Chair of its Oncology Committee and a Member of Council. He was elected Fellow of the BIR in 2007. He is author or co-author of over 100 peer-reviewed papers on various aspects of Oncology and Radiobiology.
Dr David A L Morgan began training in Radiotherapy & Oncology as a Registrar in 1977, and in 1982 was appointed a Consultant in the specialty in Nottingham, continuing to work there until his retirement in 2011. He joined the BIR in 1980 and at times served as Chair of its Oncology Committee and a Member of Council. He was elected Fellow of the BIR in 2007. He is author or co-author of over 100 peer-reviewed papers on various aspects of Oncology and Radiobiology. Andy Moloney completed his degree in Physics at Nottingham University in 1980 before joining the Medical Physics department at the Queens Medical Centre in the same city. After one year’s basic training in evoked potentials and nuclear medicine, he moved to the General Hospital in Nottingham to pursue a career in Radiotherapy Physics and achieved qualification in 1985. Subsequently, Andy moved to the new radiotherapy department at the City Hospital, Nottingham, where he progressed up the career ladder until his promotion as the new head of Radiotherapy Physics at the North Staffordshire Royal Infirmary in Stoke-on-Trent. Over the next twenty years Andy has acted as Clinical Director for the oncology department and served on the Radiation Physics and Oncology Committees at the BIR and was appointed a Fellow in 2007. He has been the author and co-author of multiple peer reviewed articles over the years prior to his retirement in 2017.
Andy Moloney completed his degree in Physics at Nottingham University in 1980 before joining the Medical Physics department at the Queens Medical Centre in the same city. After one year’s basic training in evoked potentials and nuclear medicine, he moved to the General Hospital in Nottingham to pursue a career in Radiotherapy Physics and achieved qualification in 1985. Subsequently, Andy moved to the new radiotherapy department at the City Hospital, Nottingham, where he progressed up the career ladder until his promotion as the new head of Radiotherapy Physics at the North Staffordshire Royal Infirmary in Stoke-on-Trent. Over the next twenty years Andy has acted as Clinical Director for the oncology department and served on the Radiation Physics and Oncology Committees at the BIR and was appointed a Fellow in 2007. He has been the author and co-author of multiple peer reviewed articles over the years prior to his retirement in 2017.






 A follow-up to the Unofficial Guide to Radiology, and part of the Unofficial Guide to Medicine series, this new book The Unofficial Guide to Radiology: 100 Practice Chest X-rays, with full colour annotations and full X-ray reports has at its heart the inspiring idea that the development of educational resources should be driven by those who use them. The result is a fantastic resource for reporting radiographers, medical students, junior doctors in any specialty, providing a comprehensive and practical approach to chest x-ray interpretation.
A follow-up to the Unofficial Guide to Radiology, and part of the Unofficial Guide to Medicine series, this new book The Unofficial Guide to Radiology: 100 Practice Chest X-rays, with full colour annotations and full X-ray reports has at its heart the inspiring idea that the development of educational resources should be driven by those who use them. The result is a fantastic resource for reporting radiographers, medical students, junior doctors in any specialty, providing a comprehensive and practical approach to chest x-ray interpretation. Right from the start, the book’s cover is self-explanatory and is easily perceived to be about chest X-ray interpretations. The 100 chest X-ray cases are presented in a test-yourself format, with the images and case history presented on one page and the interpretation and report on the next.
Right from the start, the book’s cover is self-explanatory and is easily perceived to be about chest X-ray interpretations. The 100 chest X-ray cases are presented in a test-yourself format, with the images and case history presented on one page and the interpretation and report on the next.


 Science is often misrepresented in the media. The BIR supports the charity Sense about Science in their call for all research to be openly and honestly reported. This year we supported one of their Voice of Young Science workshops called “Standing up for Science” held on 16 September 2016 in London.
Science is often misrepresented in the media. The BIR supports the charity Sense about Science in their call for all research to be openly and honestly reported. This year we supported one of their Voice of Young Science workshops called “Standing up for Science” held on 16 September 2016 in London. selecting and pitching stories. Science stories are selected based on interest, accessibility, and importance. These are pitched to the editors, who decide which ones to take further. The journalists pointed out that their duty is to their audience, not to science. Unfortunately, science has to compete with news on David Beckham’s haircut. Time constraints are also a problem. They write multiple articles a day (I’m three weeks and counting on this one…), so it’s important for scientists to be available to discuss their research on the day it’s published.
selecting and pitching stories. Science stories are selected based on interest, accessibility, and importance. These are pitched to the editors, who decide which ones to take further. The journalists pointed out that their duty is to their audience, not to science. Unfortunately, science has to compete with news on David Beckham’s haircut. Time constraints are also a problem. They write multiple articles a day (I’m three weeks and counting on this one…), so it’s important for scientists to be available to discuss their research on the day it’s published.