

Dr Adrian Thomas
100 years ago the UK was facing a fast-moving outbreak of epidemic influenza pneumonia, known as the “Spanish Flu”.
Radiology played an important part in diagnosis, although the crisis was without the scientific knowledge, strategic management and communications we have today. Here, Dr Adrian Thomas explores the six patterns of infection in this unpredictable and powerful disease.
Radiology is playing a central role in the diagnosis of COVID-19 today, and 100 years ago was also playing an important role in the diagnosis and characterisation of the outbreak of epidemic influenza pneumonia of 1918–1920. A combination of fluoroscopy and radiography was then used, with the occasional utilisation of stereoscopy. The greatest pointer to a diagnosis of epidemic influenza pneumonia in a given patient was the presence of the epidemic, although there were some specific features to indicate the diagnosis. The etiological cause of influenza was not known at the time, being first discovered in pigs by Richard Shope in 1931.

The epidemic of 1918 far exceeded previous ones in its intensity. It had a high mortality in young adults with the very young and very old being comparatively immune. The associated pneumonia was particularly virulent. In the case of the troopship The Olympic (sister ship of The Titanic) there were 5,951 soldiers on board. Initially there were 571 cases of acute respiratory disease, but within 3 weeks there were 1,668 cases. Of these, 32% had pneumonia, of which 59% died. In any locality the duration of the epidemic was from between 6–8 weeks, and approximately 40% of the population was affected (Osler, 1930).
Six patterns of infection were identified, with correlation of clinical, radiological and post-mortem findings (Sante, 1930., Shanks, et al. 1938). Dr Leroy Sante, the pioneer radiologist from St Louis, described epidemic influenza pneumonia as “the most lawless of the chest infections.” Abscess formation was seen frequently, and was commonly of the small and multiple type. Radiological changes were seen developing day by day, and clinical resolution needed at least six–eight weeks since there had commonly been lung destruction and healing by fibrosis needed to occur.
The patterns were:
Type 1: Peribronchial invasion with infiltrates that enlarge and become confluent forming small areas of consolidation (figures 1 & 2, below). This was not confined to one lobe, but could appear in all lobes as a true bronchopneumonia. This was similar in appearance to ordinary bronchopneumonia.

Figure 1

Figure 2
Type 2: Peribronchial invasion with infiltrates that enlarge and become confluent to form solidification of an entire lobe (figure 3, below). The changes remained confined to a single lobe. It was viewed as a true bronchopneumonia but with a lobar distribution (“pseudolobar pneumonia”). Different lobes may be invaded one after another. The pseudolobar pattern was the commonest type, and could resolve without further spread. The presence of previous isolated infiltrates would distinguish this type from common lobar pneumonia. There was a tendency to break down with extensive cavitation.

Figure 3
Type 3: This starts as blotchy infiltrates that coalesced to form a general haziness over a part of a lung, suggesting a haematogenous origin (figures 4 and 5, below). At post-mortem this was found to be an atypical lobular pneumonia, a “diffuse pneumonitis”, that was so commonly seen during the influenza outbreak. It resembled the streptococcal (septic) pneumonia that was often seen in association with septicaemia when there was no epidemic. The spread was rapid, and the prognosis was poor. Death commonly occurred within the week.

Figure 4

Figure 5
Type 4: A type starting in the hilum and spreading rapidly into the periphery, the so-called “critical pneumonia” (figure 6, below). This was attended with a high mortality. Post-mortem showed a purulent and haemorrhagic infiltration around the larger bronchi. There was often marked cyanosis.

Figure 6
Type 5: This started in the dependent part of the lungs, with continuous upwards spread (figures 7a and b, below). This was an atypical lobular pneumonia, there was no associated pleural fluid, and it was usually fatal. Initial infection in the costo-phrenic angle spread within 24 hours to involve the lower lung, and death occurred within 48 hours. Clinical features included extreme prostration, high temperature, and delirium. This pattern with rapidly advancing consolidation was seldom seen in other conditions.

Figure 7a
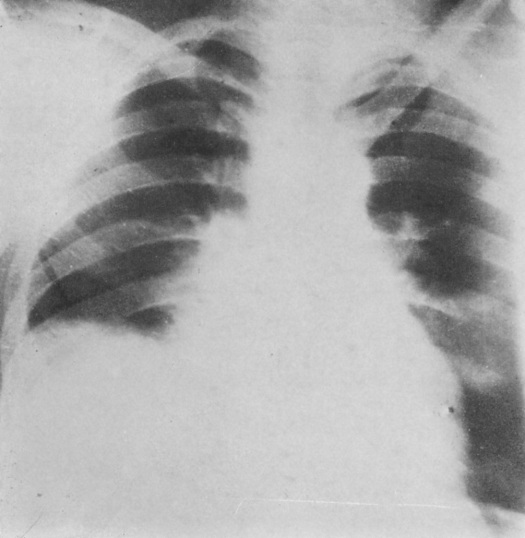
Figure 7b
Type 6. A true lobar pneumonia was only seen rarely.
The prognosis of epidemic influenza pneumonia was difficult to determine. So, as an example, a patient who was resolving would suddenly have changes extend into the other lung and then die. Another patient with successive involvement of all lobes could recover completely. A patient with only minor lung involvement might die, and another with extensive consolidation would recover completely.
Radiologists continue to be in the front line in the treatment of infectious diseases, and although our modalities are now more advanced than a century ago, their contributions remain essential. It is also noteworthy that the simple CXR also remains central.
Figures:
1. Type 1, Influenza bronchopneumonia. Image seen as a positive.
2. Type 1, Influenza bronchopneumonia. Peribronchial clusters of infiltration, with no relation to lobar architecture. Viewed as from behind.
3. Type 2, or pseudo-lobular.
4. Type 3, resembling streptococcal (septic) pneumonia. Image seen as a positive.
5. Type 3, resembling streptococcal (septic) pneumonia. Blotchy ill-defined infiltrates which coalesce to form a general haziness. Viewed as from behind.
6. Type 4, the so-called “critical pneumonia.”
7a. Type 5. This started in the dependent part of the lungs, and this early film shows consolidation in the costophrenic angle (black arrow).
7b. Type 5. A film taken 12 hours after 7a. The lower right lung is consolidated, and the patient died 12 hours later. Post mortem showed a solid lung with no effusion.
Readings:
Osler, William. (1930) The Principles and Practice of Medicine. 11th Edition, Thomas McCrae (Ed.). London: D Appleton.
Sante, Leroy. (1930) The Chest, Roentgenologically Considered. New York: Paul B Hoeber.
Shanks, S Cochrane., Kerley, Peter., Twining, Edward W. (Eds). (1938) A Textbook of X-ray Diagnosis by British Authors. London: H. K. Lewis.
Dr Adrian Thomas FRCP FRCR FBIR, BIR Honorary Historian
About Dr Adrian Thomas
Dr Adrian Thomas is a semi-retired radiologist and a visiting professor at Canterbury Christ Church University. He has been President of the Radiology Section of the Royal Society of Medicine, and of the British Society for the History of Medicine. He is the Honorary Historian to the British Institute of Radiology. He has had a long-term interest in role development in radiography, and teaches postgraduate radiographers.
Adrian has written extensively on the history of radiology writing many papers, books and articles. He has, with a colleague, written a biography of the first female radiologist and female hospital physicist: Adrian Thomas and Francis Duck: Edith and Florence Stoney, Sisters in Radiology (Springer Biographies) Springer; 1st ed. 2019 edition (1 July 2019).
© Thomas / 2020
