In the third blog of her series on AI and the radiographer, Shamie Kumar explores the impact on the radiographer when AI is integrated within an imaging modality.
In previous BIR blog posts, I have explored how AI is integrated into PACS with the AI outputs seen on radiology systems, and whether non-reporting radiographers could learn and benefit from AI. The question to explore in this blog is when AI is integrated within an imaging modality itself and how that may impact a radiographer.
AI embedded into a portable digital X-ray machine
Radiographic images are acquired in multiple modalities within different patient pathways. I will explore how AI embedded into a portable digital X-ray machine might change and affect how the radiographer works and learns.
Every radiographer is trained to take X-rays on portable machines and this is a core skill and it is an adapted technique compared with dedicated static X-rays rooms. It is unique in the sense patient positioning can vary depending on the environment and situation, whether this be on a ward or in A/E resus. Patient’s conscious level and mobility can vary, often supine and not all being cooperative. There can be situations where other healthcare professionals (HCP) are in proximity of the patient being imaged due to the image being acquired outside of the main radiology department.
AI output
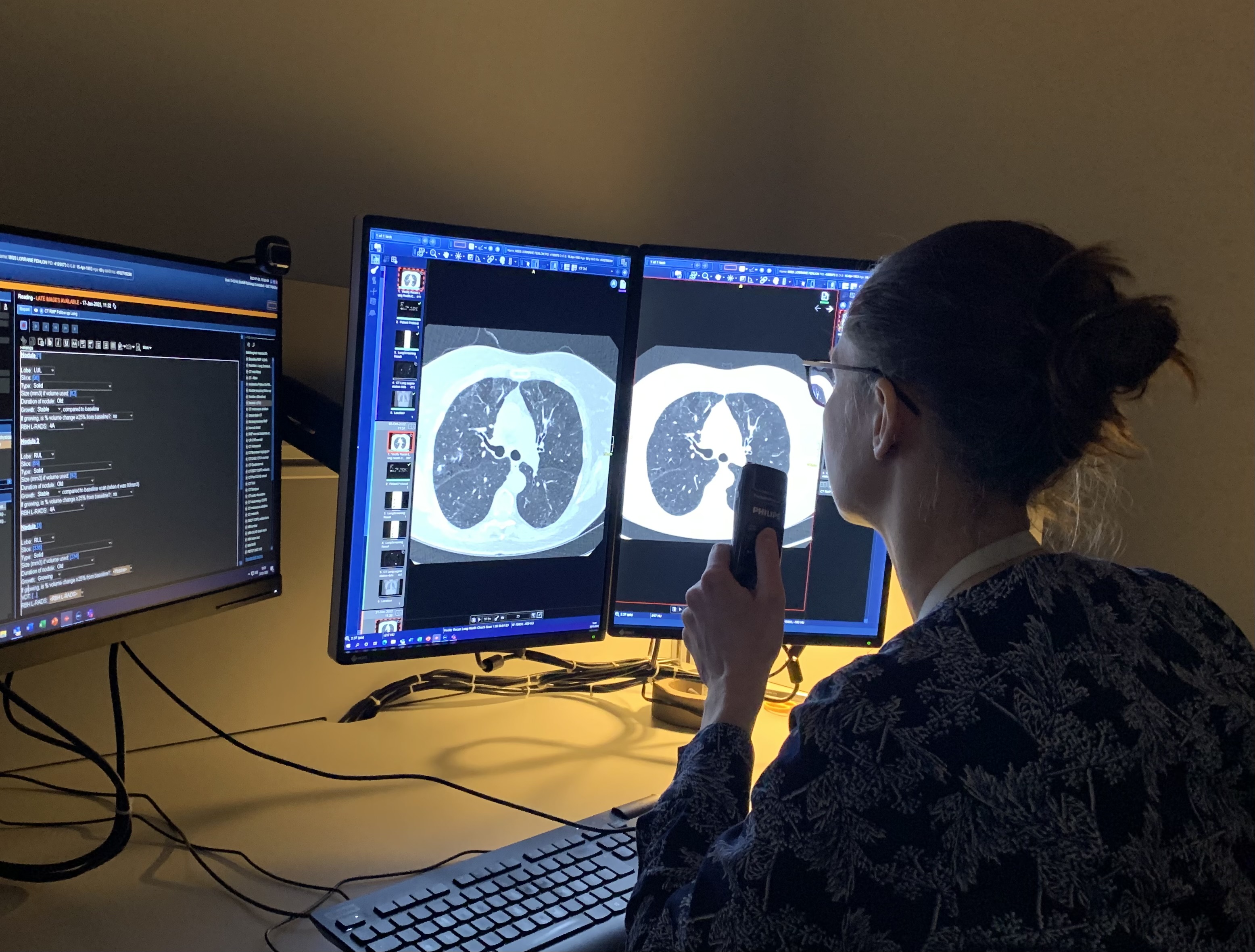
Some hospitals have adopted digital portable X-ray machines to provide an instant image, the radiographer can see the chest X-ray immediately after exposure and decide whether the image quality is optimal. As AI becomes integrated within the modality, in this instance on a portable digital X-ray machine, the radiographer will also see the AI output and findings alongside the original X-ray. Not only does the radiographer see the AI output but other HCP that are present will also have the accessibility to view the same in the given environment. As we all know, X-rays need to be reported by radiologist or reporting radiographers, but often clinicians make clinical decision before these inpatient portable x-rays reports are finalised and available on the hospital system, especially if quick intervention is required.
When AI integration is done in such a way that radiographer need not log into PACs to view the AI output and is shown on the modality once the image is acquired, all radiographers can utilise AI to its full potential. The focus quickly shifts to: does the radiographer have the relevant education and training to understand the AI intended use, the AI outputs, what are the functions, features of the AI, how do they clinically interpret these images, how does AI work and what are the limitation of AI. All these questions become important when an AI is implemented; radiographers need to be trained how to use it, become familiar with the outputs, and educate others around them. If this is approached robustly, it will empower radiographers to learn and upskill themselves with AI being part of their daily clinical workflow, giving them the confidence to support and guide other healthcare professionals (HCPs) who also are looking at the X-ray when it acquired.
AI is an assistive tool
It’s important to recognize that AI findings are never the final diagnoses. Ultimately AI is an assistive tool, embedded within portable machines. Doctors and HCPs will also view the AI output and, with time, it will be the role of the radiographers to appropriately manage and guide other healthcare professionals.
About Shamie Kumar
Shamie Kumar is a practicing HCPC Diagnostic Radiographer; graduated from City University London with a BSc Honors in Diagnostic Radiography in 2009 and is a part of Society of Radiographers with over 12 years of clinical knowledge and skills within all aspects of radiography.
She studied further in leadership, management, and counselling with a keen interest in artificial intelligence in radiology.
Following the recent BIR live event Imaging explosion across the pond – causes and solutions in which the UK and USA radiology and healthcare systems were compared, DMC Radiology Reporting co-director Professor Simon Padley reflects on the UK position.
The USA often provides a window into our own future
In the application of imaging technology, we often follow trends that emerge in the US – the rise in CT and MRI utilisation are two examples, and more recently the growth of outsourcing is following a similar trajectory.
With different healthcare models, the US does not rely on central funding to replace or add to CT and MRI capacity. NHS funding comes from the government’s general revenue, and healthcare services are provided to all residents of the UK, regardless of their ability to pay. In contrast, the US medical system is a mixed system of public and private funding. It includes a combination of private health insurance, employer-based insurance, individual out-of-pocket payments, and public programs like Medicare and Medicaid, which are funded through federal and state taxes.
In 2022 there were 6.6 million CT studies on NHS funded patients according to NHS Digital, at a time when the population was reported to be 55 million. This equates to 121 studies per 1000 of the population. In the USA this figure is more than double at 278 CT studies per 1000 of the population (84 million CT studies in a population of about 333 million CT Scans Each Year – iData Research).
And that is just CT! Official data for 2021/22 shows that between April 2021 and March 2022, NHS services in England carried out 43.8 million imaging tests across all modalities Ref. This reflects an ever-growing requirement for imaging studies to be undertaken and reported.
At the same time, the workforce needed for this activity has fallen far behind that required. We bump along the bottom of the league table for radiologists per 100,000 of the population (8.5). Europe has 13, the US 11. Couple this with complexities of pension taxation, IR35 and COVID related burnout all nudging older highly skilled and efficient radiologists towards the exit door and we have a perfect storm. Even today we have 2000 full-time consultant clinical radiologist posts unfilled across the UK. The RCR predicts a 39% workforce shortfall by 2026 (equating to 3166 full time radiologists).
This may create stress in the radiology department, but rest assured it also causes grey hair and sleepless nights for those that inhabit the carpeted management corridors. Hidden amongst every backlog of reporting there is serious pathology lying undiagnosed. When that report is provided, and the treatment options are discussed, some options will have closed, tumours will have stage shifted and outcomes will be less good. This constitutes a chief executive’s nightmare but has caught the medicolegal world’s attention. So, what are we to do?
Teleradiology and the NHS
Almost all acute trusts have turned to the services of the teleradiology community, now playing a vital role in helping to address this capacity shortfall. In the past 10 years the market has grown with a compound annual growth rate of about 10-15%.
Who are all these extra radiologists and where do they come from? Well of course, by-and-large, they are you and me. But we are a limited pool, the market rates for reporting (set by the NHS) are not great and there are only so many hours in the day.
So where can we look for additional workforce capacity and will we be allowed to access it? To allow this to happen the NHS will need to engage more readily with the solutions that are now emerging and examine the detail of how we, in the teleradiology world, are already addressing data governance and medicolegal concerns.
At DMC Radiology Reporting, we already work in partnership with many NHS Trusts. We strive to deliver fast, accurate radiology reporting with innovation and efficiency. We have a rigorous commitment to clinical governance, and we are proud of our work force of GMC-registered/FRCR-radiologists with sub-specialty interests. Like many others, we are interested in how these problems are being addressed in the US.
About Professor Simon Padley
In 2013 Simon co-founded DMC-Radiology Reporting, which has been growing and developing ever since, focusing on sub-specialist high quality outsourced reporting.
Simon is a cardiothoracic and interventional radiologist, appointed in 1994. As a previous imaging director in the NHS for many years he developed a range of new services, most recently as lead radiologist for Royal Brompton Hospital Diagnostic Imaging Centre, opened in 2022. This facility incorporates one of the only combined interventional bronchoscopy and radiology facilities in the country.
As a Professor of Practice (Diagnostic and Interventional Radiology) since 2016, at the National Heart & Lung Institute, Imperial College London, he maintains an active academic career, publishing widely with over 220 articles in peer reviewed journals.
Radiation oncology clinics face numerous challenges in the present environment, including the simultaneous management of multiple tasks (many of which are manual in nature), various degrees of standardisation, and the potential for errors to impact patient treatment. Automation can help address these challenges by reducing the time required to execute manual portions of the workflow and positively impacting the quality and safety of patient care. Tyler Blackwell, Medical Physicist discusses more:
Efficiency
To a large degree, many departments have already integrated automation into their departments. However, it stands to be a driving force of innovation in our field for the foreseeable future, coinciding with efforts to improve plan quality and reduce errors inherent in human interaction. Increasing the productivity and efficiency of our daily clinical tasks by minimizing time spent on tedious, routine tasks “below our licenses” (as worded by physicist Eric Ford as part of a Radformation Focal Spot interview) allows more time to address other critical clinical elements that require human expertise.
In developing smarter tools, we have an opportunity to improve the patient experience. Radformation CEO Kurt Sysock, MS, DABR, explains, “On average, it takes five days after simulation to create a finished plan that is ready for treatment, and we want to reduce that to less than one day.” Indeed, reducing the time between simulation and treatment can have a significant impact not only on patient satisfaction, but also on patient outcomes. Delays in treatment planning times are associated with an overall higher risk of mortality ranging from 1.2–3.2% per week for curative diseases. Reducing the time between simulation and treatment maximizes tumor control probability and patient survival.
Quality and Safety
The quality and consistency of patient care are greatly improved when the care team is able to deliver treatment as efficiently as possible. In this environment, they can devote more resources toward tasks that require greater attention or collective experience. From the clinician’s point of view, smart automation reduces the time spent on tasks that do not add value to patient care but are nonetheless important for sustaining operations.
Over the last decade, clinicians have largely embraced a culture of safety and quality improvement. This paradigm shift delivers a number of benefits for patients and involves a continued effort toward reducing errors in radiation oncology. While a number of interventions can positively influence safety and quality, automation is highly effective in this regard. Absent automation, this ongoing commitment will be inhibited by a lack of efficiency and scalability as clinicians grapple with manual processes and endless checklists.
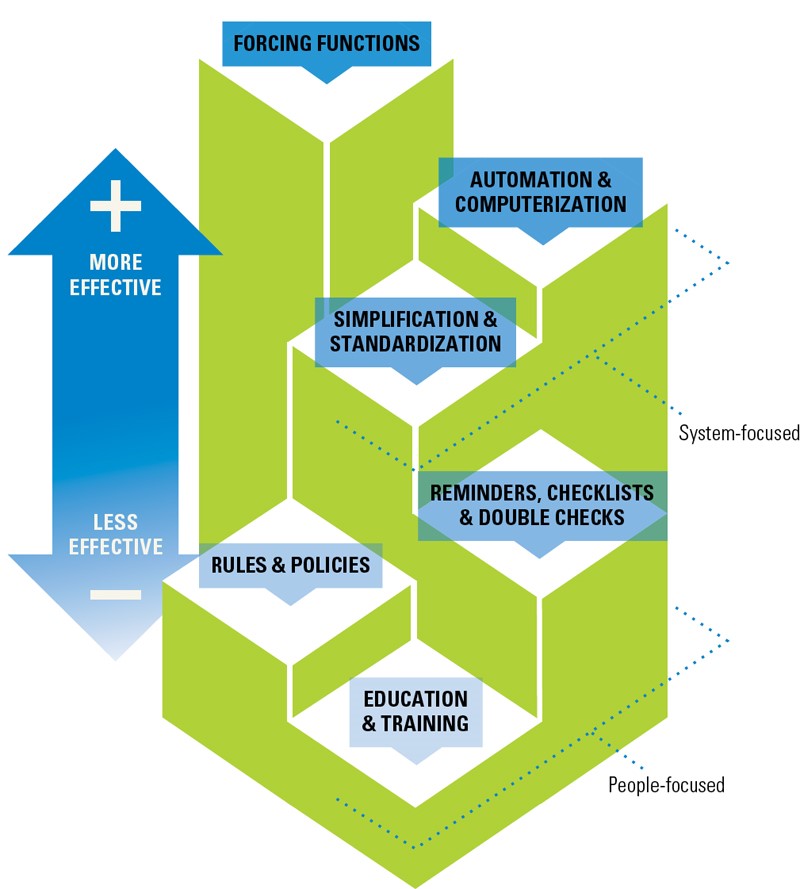
Automation is one of the most effective ways to impact change in medicine. Source: Cafazzo, J and St-Cry, O. From Discovery to Design: The Evolution of Human Factors in HealthCare. Healthcare Quarterly. April 2012. doi:10.12927/hcq.2012.22845
Automation plays a part in advances in clinical care as well. Radformation CSO Alan Nelson, DMP, DABR, argues that, “just as IMRT significantly improved the effectiveness of treatment while reducing side-effects, automation will enable the field to explore and implement new solutions for therapy protocols that otherwise simply would not have been feasible due to lack of resources.”
An Elevated Workflow At Every Step
Finding steps along the treatment care path that involve manual inputs isn’t a challenge. Wherever they exist, there is an opportunity for automation to provide value. From planning and on-treatment to billing and quality assurance, the results of these workflow improvements are impressive.
Structure Segmentation
The proper delineation of anatomical structures in the vicinity of the target is important in understanding the impact of a treatment plan on the surrounding healthy tissues. But manual contouring can be resource-intensive, and some structure boundaries—especially for target structures—can vary widely based on who is performing the work. According to physicist Noah Bice of New York University Langone, “Contouring is subjective. With any mix of individuals, there are inherently varying levels of expertise and personal preference involved.”
Within the past few years, the introduction of deep-learning algorithms for contouring has transformed the landscape. By exploiting cloud-based computational resources, structure sets, including organs-at-risk and target structures, can be generated in a fraction of the time as manual contours. Departments have been quick to adopt this new technology, which will likely become a global standard of care within the decade.
Treatment Planning
Given that every patient’s anatomy and disease state is unique, it might feel safe to assume that it may not be possible to automate this process. Despite this inherent variation, the approach to planning is algorithmic and repetitive. By scripting various repetitive processes—field-in-field or electronic compensator planning, for example—departments are capable of producing consistently high-performing plans in a fraction of the time.
This process, when applied to the Halcyon machine, has made it feasible to plan electronic compensator breast plans when otherwise manual planning is impractically cumbersome and time-consuming.
Plan Evaluation and Reporting
Determining the quality of any given treatment plan is no small task. Often, it is not easy to compare comprehensive plan quality elements within the treatment planning system (TPS). By tapping into the plan data via scripting interfaces, it’s possible to pull dosimetric information for comparison against dose constraint templates to verify the quality of a plan during or after the plan is complete.
Automated platforms are quickly becoming the standard of care, providing intuitive assessments of plan quality, including dose constraints, plan checks, machine collision risk, and reporting. While default TPS reports are often limited in scope, third-party options offer fast, customized plan reports as well as the ability to populate directly into ARIA Documents.
Comprehensive new tools allow for faster, user-friendly plan revaluation and reporting.
Quality Assurance
Collecting and sorting quality assurance information can be a challenging task given the variety of equipment and vendor products in the clinic that requires tracking. The frequency of the tasks adds another layer of complexity as well, with new data being acquired daily. Thankfully, new quality assurance platforms make short work of managing this data, providing a central location for all data from linacs and CTs to ionisation chambers and GM meters. Automation is capable of detecting new test information—from daily or monthly tests—and effortlessly syncing data to the centralized platform for quick analysis and review. These databases bring efficiency while reducing the dependency on multiple separate spreadsheets in unique locations.
Conclusion
In conclusion, the use of intelligent automation in radiation oncology—such as the solutions offered by Radformation—has the potential to revolutionize clinical workflows, leading to bottom-line improvements in patient care. By reducing the time required to execute manual portions of the workflow, clinicians can devote more time to critical clinical elements that require human expertise, such as addressing treatment planning and ensuring patient safety. Automation also plays a part in advances in clinical care and enables the field to explore and implement new solutions that may not have been feasible without this technology. In short, the benefits of automation in radiation oncology are numerous and diverse, and they can significantly enhance the overall quality and safety of patient care.
Tyler Blackwell, MS, DABR, is a medical physicist at Radformation focused on clinical collaborations and community engagement. Before joining Radformation, he spent a decade working as a clinical physicist. He is active on several committees for the American Association of Physicists in Medicine, including the board of directors, and volunteers for the American Board of Radiology.
Shamie Kumar describes how AI fits into a radiology clinical workflow and her perspective on how a clinical radiographer could use this to learn from and enhance their skills.
AI in radiology and workflow
We all know that AI is already here, actively being implemented and used in many trusts in seeing its real world value supporting radiology departments to solve current challenges.
Often this is focused on benefits to radiologist, clinicians, reporting radiographers, patients, and cost savings, but what about clinical non-reporting radiographers undertaking the X-ray or scans – can AI benefit them too?
Let’s think about how AI is implemented and where are the AI outputs displayed?
If the AI findings are seen in PACS, how many radiographers actually log into PACS after taking a scan or X-ray? Good practice is seen to have PACS open to cross-check images that have been sent from the modality. Often this doesn’t happen for various reasons but maybe it should be a part of the radiographers’ routine practice, just like post-documentation is.
Can Radiographers Up-Skill?
Given the view it does happen, radiographers will have the opportunity to look at the AI outputs and potentially take away learnings on whether the AI found something that they didn’t see initially or whether there was a very subtle finding. We all know people learn through experience, exposure, and repetition, so if the AI is consistently picking up true findings, then the radiographer can learn from it too.
But what about when AI is incorrect – could it fool a radiographer, or will it empower them to research and understand the error in more detail?
As with many things in life, nothing is 100% and this includes AI in terms of false positive and false negatives. The radiographers have the opportunity to research erroneous findings in more detail to enhance their learning, but do they actually have time to undertake additional learning and steps to interpret AI?
CPD, self-reflection, learning through clinical practice are all key aspects of maintaining your registration, and self-motivation is often key to furthering yourself and your career. The question remains: are radiographers engaged and self-motivated to be part of the AI revolution and use it to their professional benefit with potential learnings at their fingertips?
There have been a few recent publications that share insight on how AI is perceived by radiographers, what is their understanding, training and educational needs.
Many Universities like City University London and AI companies like Qure.ai are taking the initial steps in understanding this better and taking active efforts in filling the knowledge gap, training and understanding of AI in radiology.
Radiographers who are key part of any radiology pathway, are yet to see the real-world evidence on whether AI can upskill radiographers, but there is no doubt this will unfold with time.
About Shamie Kumar
Shamie Kumar
Shamie Kumar is a practicing HCPC Diagnostic Radiographer; graduated from City University London with a BSc Honors in Diagnostic Radiography in 2009 and is a part of Society of Radiographers with over 12 years of clinical knowledge and skills within all aspects of radiography. She studied further in leadership, management, and counselling with a keen interest in artificial intelligence in radiology.
References
Akudjedu, T. K. K. N. M., 2022. Knowledge, perceptions, and expectations of Artificial intelligence in radiography practice: A global radiography workforce survey. Journal of Medical Imaging and Radiation Sciences.
Coakley, Y. M. E. C. M. M., 2022. Radiographers’ knowledge, attitudes and expectations of artificial intelligence in medical imaging. Radiography International Journal of Diagnostic Imaging and Radiation Therapy, 28(4), pp. P943-948.
Malamateniou, K. P. W. H., 2021. Artificial intelligence in radiography: Where are we now and what does the future hold?. Radiography International Journal of Diagnostic Imaging and Radiation Therapy, 27(1), pp. 58-62.
Cheryl Cruwys, European Education Coordinator at DenseBreast-info.org/Europe, highlights the importance of understanding the screening and risk implications of dense breast tissue. DenseBreast-info.org’s mission is to advance breast density education and address the gap in knowledge about dense breasts.
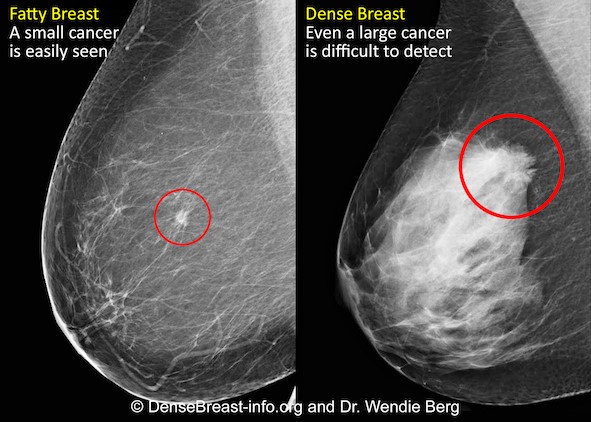
Mammography remains the standard of care in screening for breast cancer and has been proven to reduce the mortality rate [1]. However, in dense breasts, cancers can be hidden/obscured on mammography [2,3] (Fig.1) and may go undetected until they are larger and more likely to present with clinical symptoms [4]. Breast density has also been identified as the most prevalent risk factor for developing breast cancer [5].
Women with dense breasts are BOTH more likely to develop breast cancer and more likely to have that cancer missed on a mammogram [5]
Fig. 1 – Cancer on a mammogram of a fatty vs a dense breast
What is Dense Breast Tissue?
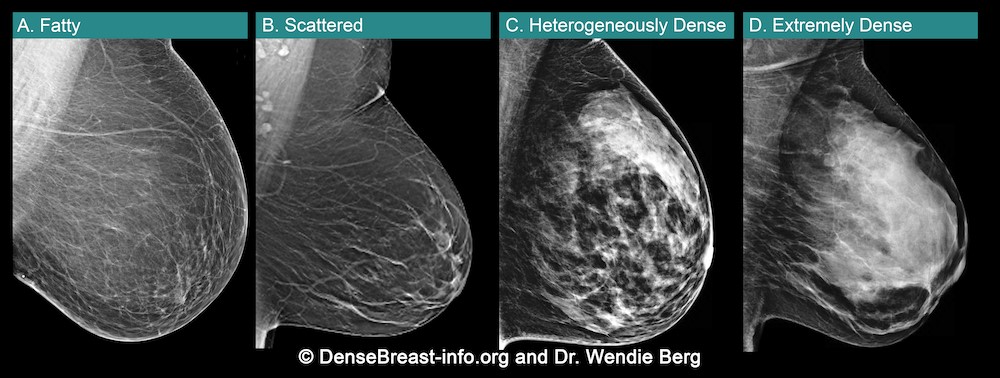
Breasts are made of fat and glandular tissue, held together by fibrous tissue. The more glandular and fibrous tissue present, the “denser” the breast. Breast density has nothing to do with the way breasts look or feel. Whilst dense breasts are normal and common, dense breast tissue makes it more difficult for radiologists to detect cancer on a mammogram.
Breast density is determined through a mammogram and described as one of four categories (Fig. 2), (A) Fatty, (B) Scattered, (C) Heterogeneously Dense, (D) Extremely Dense. Breasts that are (C) heterogeneously dense, or (D) extremely dense are considered “dense breasts”. Fig. 2
Figure 2
Dense Breasts Facts
40% of women over age 40 have dense breasts.
Dense breast tissue is an independent risk factor for the development of breast cancer; the denser the breast, the higher the risk.
Mammograms will miss about 40% of cancers in women with extremely dense breasts.
Women with extremely dense breasts face an increased risk of late diagnosis of breast cancer.
In these women, screening tests, such as ultrasound or MRI, when added to mammography, substantially increase the detection of early-stage breast cancer.
Dense Breast Educational Resources
DenseBreast-info.org/Europe is the world’s leading website about dense breasts. This medically-sourced resource is the collaborative effort of world-renowned experts in breast imaging and medical reviewers. Fig 3.
Figure 3
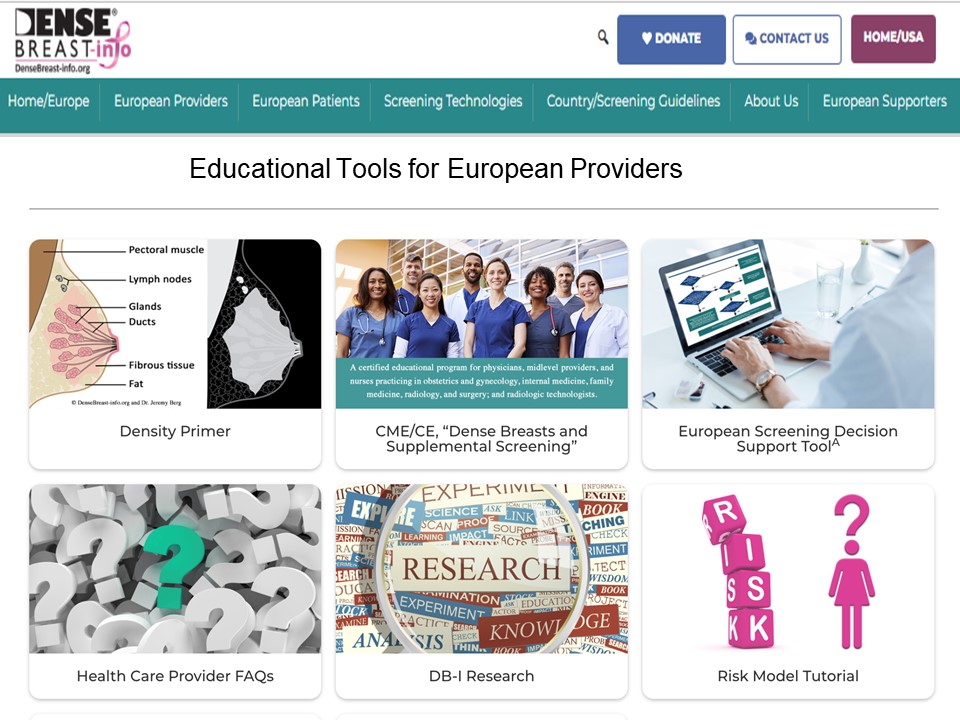
The website features educational tools for both European Patients and Providers Fig. 4. (a and b)
Figure 4 (a)
CME Course – Learn Why Breast Density Matters!
The DenseBreast-info.org resource includes a free CME/CE course, Dense Breasts and Supplemental Screening suitable for primary care healthcare providers, including family medicine, internal medicine, and OB/GYN physicians and midlevel providers, as well as radiologists, and radiologic technologists (UEMS-EACCME® mutual recognition for AMA credits).
A growing number of medical organisations link to the DenseBreast-info.org website, including the EFRS (European Federation of Radiographer Societies) and the Society of Radiographers.
Figure 4 (b)
The website includes breast screening guidelines in Europe. A comparative analysis table summarises the guidelines in each country.
NHS Breast Screening Programme
Currently in the UK, population routine screening mammograms are offered to women aged 50–74, every 3 years. Though dense breasts affect the likelihood that a cancer will be masked and increases a woman’s risk for developing breast cancer, it is not part of UK data collection. A woman’s breast density is not assessed, not recorded in medical records, nor reported to her. For diagnostic purposes, this may differ. However, in many other European country screening programs, a woman’s breast density is assessed, recorded, and the woman’s personal breast density category is included in the mammography report.
News in Europe: the EUSOBI Recommendations
Population based breast screening guidelines vary across Europe. In the UK, asymptomatic women attending routine national breast screenings receive mammography alone. In some countries (e.g., Austria, Croatia, Hungary, France, Serbia, Spain, Switzerland) screening guidelines for women with dense breasts include that they be offered supplement ultrasound following a mammogram.
Following recent MRI screening trials there is cumulating evidence which confirms that women with dense breasts are underserved by screening with mammography alone [7,8]. In March 2022, new guidelines were issued in Breast cancer screening in women with extremely dense breasts by the European Society of Breast Imaging (EUSOBI) [9] highlighting the growing evidence, particularly the results of a randomised, multicentre controlled study, the Dense Tissue and Early Breast Neoplasm Screening (DENSE) Trial. [7,8]
The European Society of Breast Imaging 2022 recommendations now step away from the one-size-fits all approach of mammography that is currently adopted by most European screening organizations and advocates for tailored screening programmes. There is compelling evidence that the new recommendations enable an important reduction in breast cancer mortality for these women.
Summary of the EUSOBI Recommendations
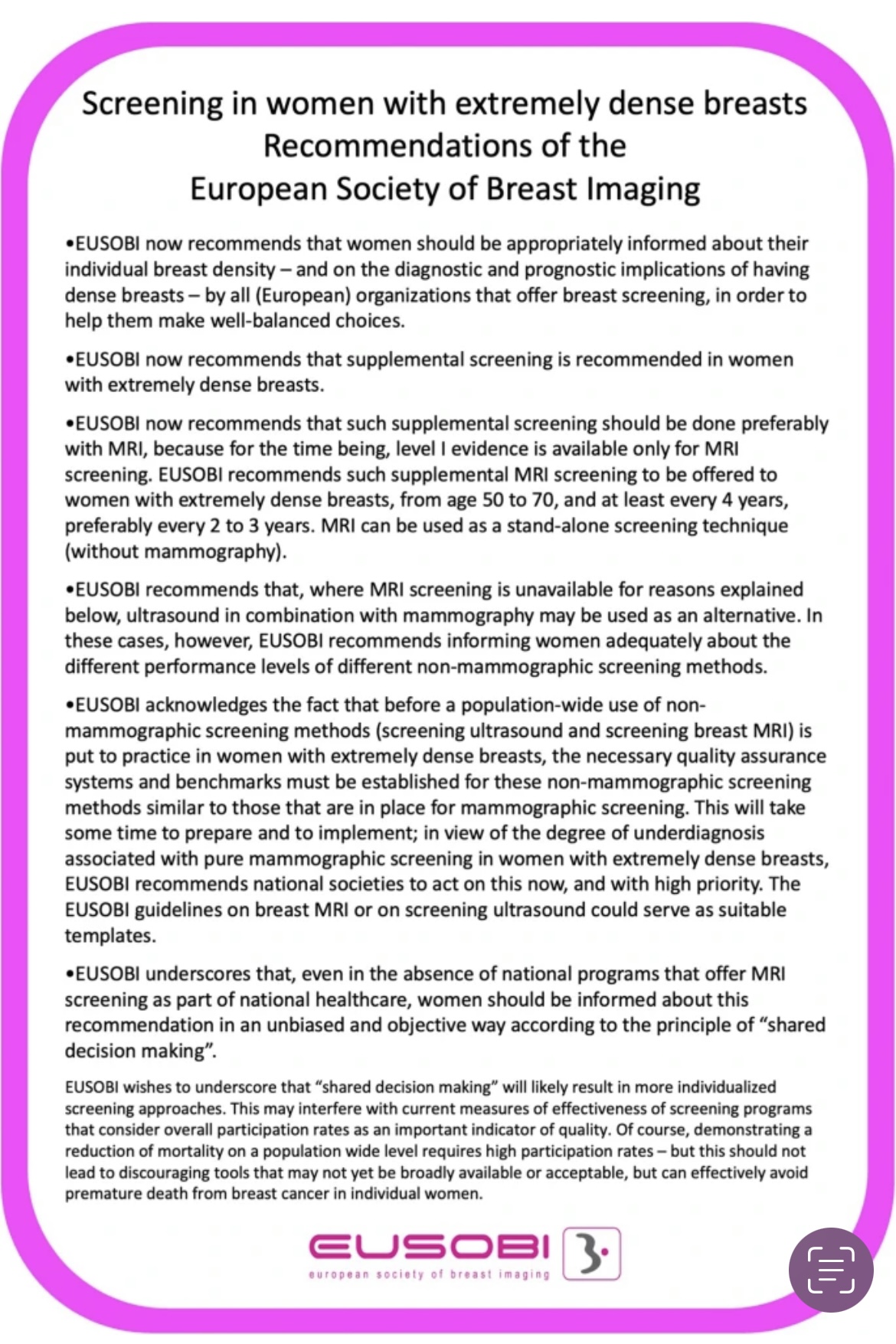
Below is EUSOBI’s summary graphic of the recommendations (Fig. 7) that highlight:
Supplemental screening is recommended for women with extremely dense breasts.
Supplemental screening should be done preferably with MRI …. where MRI is unavailable… ultrasound in combination with mammograph may be used as an alternative.
In addition to recommended additional screening in women with extremely dense breasts, note that EUSOBI recommends that“women should be appropriately informed about their individual breast densityin order to help them make well-balanced choices.”
EUSOBI acknowledges that it may take time before the new recommendations are implemented in Europe and that the level of implementation is dependent on the resources that are available locally.
It is important to emphasize that the EUSOBI recommendations highlighted in this article are not yet guidelines in Europe. Of course, it is hoped that in Europe, national breast screening committees try to implement these recommendations as soon as possible to benefit women.
Figure 7
World Dense Breast Day Success!
DenseBreast-info.org launched the first #WorldDenseBreastDay on 28 September 2022.
Nearly 100 posts with great images were created and ran for 24 hours across social media channels. Analytics detailed participation from people in 37 countries, over 8.6 million people saw/read the posts and over 17,000 people interacted with the posts.
The purpose of the day is to raise awareness about dense breasts and share medically-sourced educational resources available for women and health providers.
Please join us next year for #WorldDenseBreastDay which will take place on 27 September 2023!
Take Home Message:
Breast density can both hide cancers on a mammogram and increases the risk of developing breast cancer.
Women with dense breasts benefit from additional screening tests after their mammogram
Breast density education and access to supplemental screening can mean the difference between early- or late-stage diagnosis
Physicians should be educated and prepared to have patient conversations about breast density
1, Tabar L, Vitak B, Chen T H et al. Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology 2011;260:658-63
2. Hooley RJ, Greenberg KL, Stackhouse RM, Geisel JL, Butler RS, Philpotts LE (2012) Screening US in patients with mammographically dense breasts: initial experience with Connecticut Public Act 09-41. Radiology 265:59–69
3. Kolb TM, Lichy J, Newhouse JH (2002) Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology 225:165–175
4. RoubidouxMA, Bailey JE,Wray LA, HelvieMA(2004) Invasive cancers detected after breast cancer screening yielded a negative result: relationship of mammographic density to tumor prognostic factors. Radiology 230:42–48
5. McCormack VA, dos Santos Silva I (2006) Breast density and parenchymal patterns as markers of breast cancer risk: a metaanalysis. Cancer Epidemiol Biomarkers Prev 15:1159–1169
6. Vourtsis A, Berg W A. Breast density implications and supplemental screening. Eur Radiol 2019;29:1762-77.
7. Bakker M F, de Lange S V, Pijnappel R M et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med 2019;381:2091-102.
9. Mann, R.M., Athanasiou, A., Baltzer, P.A.T. et al. (2022) Breast cancer screening in women with extremely dense breasts recommendations of the European Society of Breast Imaging (EUSOBI) Eur Radiol 32, 4036–4045
Cheryl Cruwys is a British breast cancer patient, advocate, author and educator. While living in France (2016) she was diagnosed with early-stage breast cancer and credits the early detection of breast cancer to the French standard practice of performing supplemental screening on dense breast tissue. She is founder of Breast Density Matters UK, European Education Coordinator at DenseBreast-info.org/Europe, a member of the European Society of Radiology Patient Advisory Group and a Patient Rep on the ecancer.org Editorial Board.
Cheryl works at the European level with patient advocacy and medical societies, attends/presents at key scientific symposiums and works with international breast imaging experts to disseminate education on dense breasts. DenseBreast-info.org
We are all familiar with the concept of artificial intelligence in radiology and its application that is expanding rapidly. But how will AI in the workplace affect the radiographer and how does it differ from the red dot system radiographers are so familiar with?
Shamie Kumar describes her perspective on how radiography has evolved over time, the impact radiographers can have in detecting abnormal X-rays and reflects how she views fast approaching AI in advancing current skills.
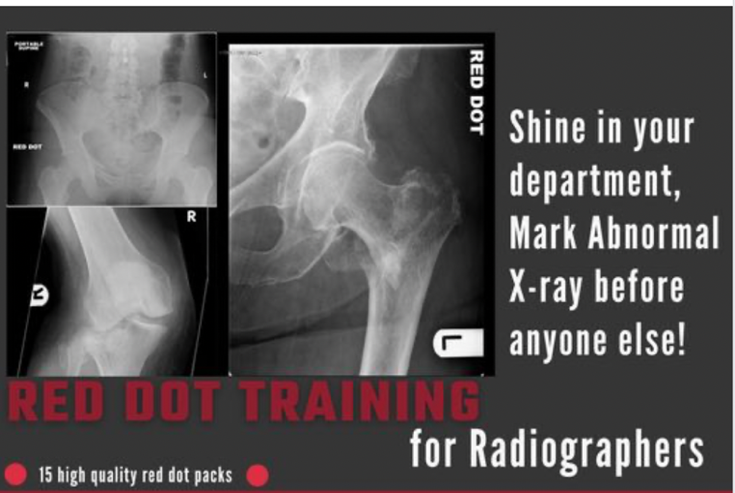
The Red Dot System
Often one of the first courses a newly qualified radiographer attends is the red dot course. This course demonstrates pathologies and abnormalities often seen in X-rays some obvious, others not, giving radiographers the confidence to alert the referring clinician and/or radiologist that there is something abnormal they have seen.
The red dot system is a human alert system, often two pairs of eyes are better than one and assist with near misses. How this is done in practice can vary between hospitals, in the era of films the radiographer would place a red dot sticker on the film itself before returning it to clinician or radiologist. In the world of digital imaging this is often done during “post documentation” a term used once the X-ray is finished, the radiographer will complete the rest of the patient documentation to suggest the X-ray is complete, ready to be viewed and reported. As part of this process the radiographer can change the status of the patient to urgent along with a note for what has been observed. From this the radiologist knows the radiographer has seen something urgent on the image and the patient appears at the top of their worklist for reporting and, so the radiologist can view the radiographer’s notes.
The Role of AI in Radiology
Artificial Intelligence (AI) is moving at a pace within healthcare and fast approaching radiology departments, with algorithms showing significant image recognition in detecting, characterisation and monitoring of various diseases within radiology. AI excels in automatically recognising complex patterns in imaging data providing quantitative assessments of radiological characteristics. With the numbers for diagnostic imaging requests forever increasing, many AI companies are focusing on how to ease this burden and supporting healthcare professionals.
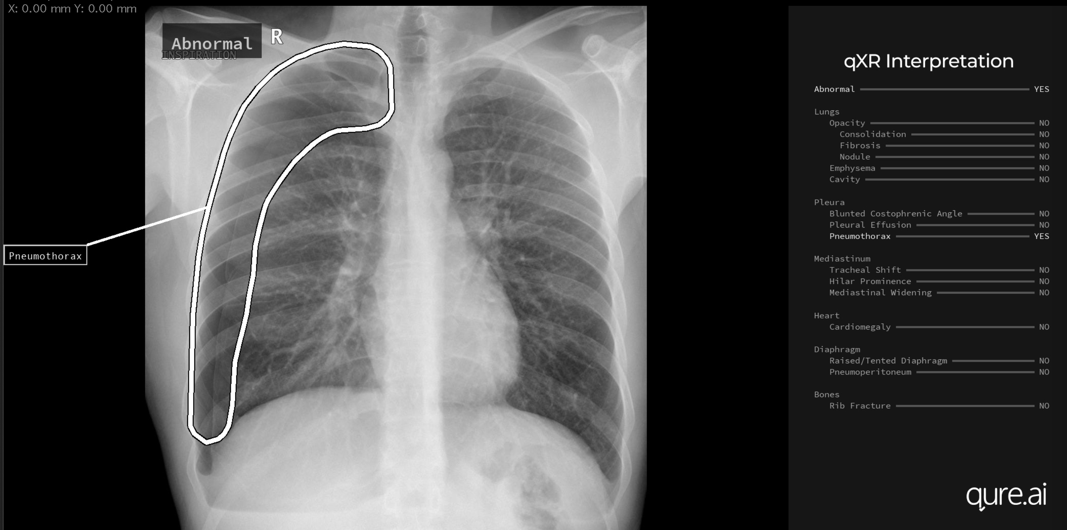
AI triage is done by the algorithm based on abnormal and normal findings. This is used to create an alert for the referring clinician/radiologist. It can be customised to the radiologist, for example colour-coded flags, red for abnormal, green for normal, patients with a red flag would appear at the top of the radiologist worklist. For the referring clinicians who don’t have access to the reporting worklist, the triage would be viewed on the image itself with an additional text note suggesting abnormal or normal.
Image courtesy of qure.ai
What does AI do that a radiographer doesn’t already? AI is structured in a way that it gives the findings; for example, a pre-populated report with its findings or an impression summary and its consistent without reader variability. So, the question now becomes what can AI do beyond the red dot system. Here, the explanation is straightforward. Often a radiographer wouldn’t go to the extent of trying to name what they have seen, especially in more complex X-rays like the chest where there are multiple structures and pathologies. For example, a radiographer would mention right lower lobe and may not go beyond this, often due to confidence and level of experience.
AI can fill this gap; it can empower radiographers and other healthcare professionals with its classification of pathologies identifying exactly what has been identified on the image, based on research and training of billions of data sets with high accuracy.
The radiographers may have the upper hand with reading the clinical indication on the request form and seeing the patient physically, which undoubtably is of significant value. However, the red dot system has many variables specific to that individual radiographer’s skills and understanding. It is also limited to giving details of what they have noted to just the radiologist. What about the referring clinician who doesn’t have access to the radiology information system (RIS) where the alert and notes are? Do some radiographers add a text note on the X-ray itself?
Summary
Yes, AI is a technological advancement of the red dot system and will continue to evolve. It is structured in how it gives the findings and does this consistently with confidence adding value to early intervention, accurate patient diagnosis, contributing to reducing misdiagnosis and near misses. AI is empowering radiographers, radiologists, referring clinicians and junior doctors by enhancing and leveraging their current knowledge to a level where there are consistent alerts and classified findings that can even be learned from. This doesn’t replace the red dot system but indeed enhances it.
The unique value a radiographer adds to the patient care, experience and physical interaction can easily be supplemented with AI, allowing them to alert with confidence and manage patients, focusing the clinician time more effectively.
About Shamie Kumar
Shamie Kumar is a practicing HCPC Diagnostic Radiographer; graduating from City University London, BSc Honors in Diagnostic Radiography in 2009 and part of Society of Radiographers with over 10 years of clinical knowledge and skills within all aspects of radiography. She studied further in leadership, management and counselling with a keen interest in artificial intelligence in radiology.
Steve Holloway, from Signify Research explores the daunting challenge of navigating the road to Enterprise Imaging.
Cloud technology is transforming how we live and work today. For healthcare providers undergoing long-term digitalisation, the potential of cloud technology resonates, yet the complexities of adoption are daunting and difficult to navigate. Nowhere is this more evident in healthcare than imaging informatics.
A front-runner of healthcare digital innovation, the imaging sector has a complex legacy of on-premise, siloed, best-of-breed applications that interact with and influence every point of the care continuum.
Many providers have taken the positive steps of embarking on an enterprise imaging strategy, federating imaging service line applications, centralising data management and transforming access for diagnosticians, care givers, and patients.
Progress on this mission has been challenging however, in part due to an over-reliance on aging on-premise applications and limited availability of alternatives.
Today, a new generation of cloud-based enterprise imaging solutions is emerging, offering a tangible route to cloud. In this paper, we’ll identify the key characteristics of this new generation of cloud-based products and outline the key drivers and barriers to their adoption.
Further, we’ll describe the long-term transformative power that cloud offers for enterprise imaging and the future of healthcare provision, providing our view on the key considerations for providers navigating cloud adoption for enterprise imaging.
One of the first doctors to use radiology to diagnose diseases of the nervous system, Artur Schüller began his first systematic survey of the skull just a few years after X-rays were first discovered. Here, Andrew Schuller, a distant cousin, describes his extraordinary academic and personal journey which led to his recognition as the “Father of Neuroradiology”.
Artur Schüller (hereafter Arthur Schuller) was born in the Moravian city of Brunn (now Brno in the Czech Republic) in 1874. Most of the Schullers in Brunn were involved in the textile industry but Arthur’s father, Jonas, was an ENT specialist. Arthur did well at the German-language secondary school and went on to enrol in the medical school of the University of Vienna, which at that time had an excellent international reputation. He graduated in 1899 sub auspiciis Imperatoris, a rare title only awarded by the Emperor to students who had scored perfect marks in all their school and university exams. This entitled him to select his post-graduate mentors and Arthur chose Wagner-Jauregg and Kraft-Ebbing, a combination that matched his interest in both anatomy and psychiatry. They sent him off to Berlin for 6 months in 1901 where he worked with Munk, Oppenheim and Krause who taught him about experimental physiology, clinical neurology and the diagnosis and treatment of brain tumours. By the time Schuller returned to work at the Allgemeine Krankenhaus, Vienna had already taken up Roentgen’s 1896 discovery of X-rays and Arthur was soon working with Guido Holzknecht, leader of Vienna’s radiological research efforts.
Arthur Schuller
Schuller was the first to describe the role of X-ray in diagnosing diseases of the nervous system. Working with dried skulls from the museum and with live patients his painstaking analysis of countless X-rays enabled him to produce the first systematic survey of the radiology of the skull, which described both normal and pathologic anatomy. This book The Skull base on the Radiogram (Die Schädelbasis im Röntgenbilde: Archiv und Atlas der Normalen und Pathologische Anatomie) was published in 1905 and was followed in 1912 by Röntgen-Diagnostik der Erkrankungen des Kopfes (Röntgen Diagnosis of Diseases of the Head) which encapsulated his extensive work on a range of topics and was eventually translated and published in 1918 by C V Mosby in America under the auspices of the US Army (Incidentally, during WW2 Schuller, by that time in Australia, wrote about battlefield head injuries and worked in a military rehabilitation hospital).
Schuller’s interests ranged widely. From 1904 he was Director of the Children’s Hospital where he had worked in both the Neurology and the Psychiatric Clinics. But he maintained his experimental lab work and practice at the Allgemeine Krankenhaus. By 1907 he not only passed his Habilitation (PhD) but was also awarded Dozent status which allowed him to teach courses at the university as well as privately; he kept an X-ray machine in his home. When he was made a University Professor in 1914 he was the youngest in the medical faculty. In addition to his contributions to neurosurgical procedures (transsphenoidal approach to the pituitary, antero-cordotomy and hydrocephalic drainage) Schüller is associated with three bone diseases: the Hand Schüller Christian syndrome, osteoporosis circumscripta and cephalohaematoma deformans. But it is in his foundational work in forming the discipline of Neuroradiology that his outstanding contribution lies.
The financial stringencies and the political volatility that followed the collapse of the Austro-Hungarian Empire in 1918 had a serious impact on the ability of the Vienna Medical School to maintain its position at the forefront of medical research. But the continuing presence of so many prominent medical scientists enabled it to retain its international reputation. Along with Wagner-Jauregg Schuller was instrumental in expanding the existing post-graduate courses which attracted students from round the world. The US even established The American Medical Society of Vienna to administer the flow of almost 12,000 American students who enrolled in these courses between 1921 and 1938. Schuller continued to write papers and teach but he also consolidated his international reputation by travelling the world to lecture at conferences and clinics in the UK, Europe, Latin America and the US, where he lectured at the universities of Chicago, Johns Hopkins and New York and the Mayo clinic. In teaching and travelling he established strong personal contacts that would stand him in good stead including both Harvey Cushing and Walter Dandy in the US, both pioneering neurosurgeons with an interest in radiology. In 1935, while attending the Second International Neurological Congress in London, he met Hugh Cairns, an Australian neurosurgeon, who invited him to come to Oxford. Perhaps the apex of Schuller’s career was the central role he played in the first international congress of neuroradiologists. This, the First Symposium Neuroradiologicum was held in Antwerp in July 1939; the 22nd symposium will be held in 2022. There are some who assert that it was the Swede Lysholm who really established neuroradiology by developing contrast radiography, though it was Dandy who first wrote about ventriculography.
Schuller may not have pursued contrast radiography because of the lack of research facilities in interwar Vienna or because of the eclecticism and breadth of his intellectual interests but there is no doubt that his work was foundational for the routine radiography of the sella and its environs and the diagnosis of pituitary tumours. At the eighth Symposium Neuroradiologium in 1967 Bull and Fischgold declared “Without a shadow of doubt Arthur Schuller was the father of neuroradiology”. Schuller’s papers are still quoted in current literature and the Austrian Neuroradiological Society awards and annual Arthur Schüller Prize.
The Antwerp Symposium 1939
Schuller’s private life also flourished. In 1906 he had married Margarete Stiassni from a family of successful textile industrialists in Brunn. Arthur and Margarete were introduced at a post-opera supper party at the Sacher Hotel in Vienna where they shared their love of music. Arthur was a very competent violinist and played in the Vienna Medical School orchestra. In spite of the unsettled political situation, Vienna’s cultural life was still extraordinarily rich and the Schullers participated actively. They lived in a flat close to the university and the hospital and owned a house in Brunn and a weekend cottage by the Danube north of Vienna. They had a comfortable though not extravagant lifestyle. Indeed, the son of Arthur’s urologist cousin Hugo Schuller, who lived round the corner, reported that Arthur and Margarethe were somewhat parsimonious. Their two sons were born in 1908 and 1909. It may be that dedication to Arthur’s profession and his travel schedule had some impact on his relationship with Franz and Hans. It seems that they were closer to their mother’s family in Brunn than to the other Schullers in Vienna. They spent at least some of their teenage years living in Brunn with Margarete’s mother, to whom they were devoted, and both decided to join the family business rather than go to university, with fateful consequences.
Arthur’s 60th birthday. Grandmother and sons are highlighted. Arthur Schuller is 5th from right and his wife Margarete is 6th from right.
The unstable political situation in Vienna deteriorated further in the late 1930s and after the Anschluss in March 1938 life for Jews became very difficult. Although Arthur and Margarete had been baptised as Roman Catholics in 1908 the National Socialist decrees categorized them as Jews. As such Arthur was only allowed to treat other Jews and in April 1938 he was officially “sent on holiday” from the university along with more than half of the members of the Medical Faculty, a purge that effectively set the Vienna Medical School back 60 years. The Nazi rampage through Vienna in November 1938 persuaded the Schullers that it was time to leave. Dandy had invited them to go to the US but Arthur was concerned about growing anti-semitism in academic medical circles there and decided on Australia. It seems that he was encouraged by two Australians who had attended his courses in Vienna and were now significant figures in Australian medical circles. Both John O’Sullivan and Sydney Sunderland were in Oxford in 1939 and to Oxford was where the Schullers fled when their Australian visas and their German Reich passports and exit papers arrived in early 1939. Arthur had followed up on Cairns’ invitation and in April was welcomed and attached to the labs of Le Gros Clark in Anatomy and Barclay at the Nuffield Institute for Medical Research. While there Oxford Arthur wrote a paper on the sub-arachnoid cisterns and their demonstration using a positive contrast agent which was published in BJR in 1940, 13.(148):pps 127-29
The Symposium in Antwerp finished on 29 July, 1939 and in the first week of August the Schullers left Croydon airport on a KLM flight which took over a week and 30 stops to reach Darwin and then Brisbane and eventually on to Melbourne. Their arrival was noted in the press in the main Australian cities.
What the Australians had organised was a position at St Vincent’s Hospital in Melbourne run by the Sisters of Charity, which is where John O’Sullivan was based in the Radiology Department. Also at St Vincent’s was Frank Morgan the first specialist neurosurgeon in Australia. Schuller enjoyed spending time in both departments viewing and reporting on all head X-rays and attending Morgan’s ward rounds and operations. He was liked and respected by staff at all levels. Curiously, however, the Medical Board of Victoria did not recognise his University of Vienna qualifications and he was not formally permitted to practise in Victoria till 1946. He was lent rooms where he did see patients who were referred to him. He continued to write papers – his last was published in 1950 – and, although he declined to attend the second Symposium Neuroradiologicum in Rotterdam in 1949, he was elected Honorary President and the paper he submitted was given pride of place.
Dr Schuller and Dr Frank Morgan
In spite of his age Schuller’s attendance at St Vincent’s was constant, falling off only in his eighties. It was also stoical since on top of beginning to suffer from Parkinsons he had to bear the personal sorrow of family tragedy. Although they could have escaped, the Schullers’ two sons decided to stay in Brunn partly to care for their grandmother and partly to try to rescue the Stiassni family business. Both of them along with their grandmother and Hans’ wife and young daughter perished in Auschwitz in early 1943, though this news did not reach Australia till 1945. Arthur became increasingly depressed and even asked Morgan to perform a frontal lobotomy which Morgan refused to do. Arthur died in 1957 aged 83.
Margarete survived till 1971. She had taken to offering her services as a domestic help and, as such, worked for a number of Melbourne families. She cooked, ironed and looked after children. It is not clear why she did this. Since she left a substantial estate and her brother had continued to send monthly remittances from the USA financial need was probably not her main motivation. More likely she needed social company. She certainly embedded herself in some of the families for whom she worked. She was a devoted member of her local Catholic Church community.
Members of two of those families are featured in a 30 minute documentary film about the Schullers which is available for free viewing on YouTube at https://youtu.be/YhRLobn-Ubw
Also featured is Dr Keith Henderson who, as a young neurosurgeon at St Vincents, worked with and befriended Arthur. Henderson wrote a biographical memoir of the Schullers entitled Arthur Schuller Founder of Neuroradiology: a Life on Two Continents which Hybrid Publishers in Melbourne have just, in February 2021, published posthumously *. Henderson’s book contains substantially more detail about Schuller’s contributions to medical science than the film and it lists about half of the 300 papers he published.
Andrew Schuller was born in and educated at Oxford. He worked for over 30 years for Oxford University Press in New York and Oxford. Now retired, he spends much of the year in Australia and continues to be engaged in some publishing projects as well as family history. Andrew’s grandfather was a first cousin of Arthur Schuller, though it is not known if they ever met. By a strange series of coincidences, Andrew became involved in helping Keith Henderson in the writing of his memoir. It was at the suggestion of Austrian historians who have been recording the career and fate of Jewish medical practitioners in Vienna that Andrew embarked on making the film. He regrets that he did not know about Arthur much earlier when it would have been possible to talk to more people who knew him in Austria, Oxford and Australia.
Over the last 18 months, GenesisCare has treated more than 170 patients on the UK’s first ViewRay MRIdian MR-linac and adopted SMART planning as a new way of working. Here, Ben George explains why this latest hypofractionated technique has proven to be one of the success stories of the COVID-19 era.
Stereotactic ablative radiotherapy (SABR) is growing in importance in the curative cancer pathway. Increasingly, it offers patients the opportunity to enjoy relatively long periods of disease control where previously they would have been considered for palliative treatments. During COVID-19, the scales have tipped even further in favour of hypofractionated techniques because protocols have been revised to limit the risk of patient infection. More recently, attention has turned to stereotactic ablative MR-guided adaptive radiotherapy (SMART) – the most exciting development in radiotherapy for years, with the potential to treat previously inaccessible targets.
GenesisCare has been the first in the UK to adopt SMART, installing the first ViewRay MRIdian MR-linac just over a year ago. Since then, we have treated over 170 patients, some of which are the most challenging in the world from a radiotherapy perspective, such as pancreatic, central lung and now renal cell carcinomas. MRIdian sits within our SABR offering, which is run by a specialist team of oncologists, physicists, dosimetrists, and radiographers. Over an intensive 18 months, we have adopted a completely new way of working and overcome the challenges of a pandemic to treat patients not just from across the UK, but also from around the world.
SMART explained
The MRIdian MR-linac combines a 0.35 T split superconducting magnet with a 6 MV linear accelerator. This gives it unique advantages over conventional external beam radiotherapy linear accelerators, which rely on kV cone-beam CT (CBCT) imaging, and enables an entirely new approach to treatment.
First, using MRI instead of CBCT provides superior soft-tissue visualisation. This increased imaging capability allows the treatment to be adapted at each fraction based on the daily position of the target and nearby organs at risk (OARs). This is in marked contrast to external beam treatment with CBCT, where anatomy captured in the CBCT is simply rigidly matched against a planning CT. This rigid registration is then used to calculate the movements required to shift the patient into the correct position for treatment.
Second, the MRIdian takes images continuously throughout the treatment period to not only monitor the patient position, but also turn the treatment beam on and off. This is carried out as the patient’s anatomy moves through the breathing cycle.
This combination of enhanced visualisation and real-time imaging adds a layer of certainty in the delivery of treatment.
The MRIdian on-table adaptive planning system generates a new, optimised treatment plan for each fraction. This accounts for these day-to-day anatomical variations when the patient is in the treatment position.
Treatment delivery is then automatically gated so that the dose is only delivered when the target is in the optimal position. The machine is able to monitor every intrafraction motion caused by breathing or organ-filling.
As a result of these factors, we can design plans which deliver a higher dose, more precisely than with conventional SABR. There is no need for invasive fiducial marker insertion and any uncertainty is removed. Moreover, we can reduce planning target volumes, remove internal target volumes, and minimise the amount of tissue irradiated.
SMART has led to a paradigm shift in how some cancers are treated. In particular, it can benefit cancers in areas where there is significant inter- or intrafraction motion of either the target or OARs. Across the global community, MR-linac centres are now treating novel indications, such as renal, central lung and hepatobiliary tumours, and achieving clinical outcomes not previously thought possible. It is not simply a case of improving on an existing treatment – for some tumour types, SMART is facilitating new referral patterns for patients who may not typically be eligible for radiotherapy.
Pancreatic cancer – a new way of treating
Pancreatic cancer is one such example and of all the tumour sites we are now treating at GenesisCare, this is undoubtedly the one that is breaking most ground, offering new hope for both clinicians and patients.
For decades, surgical resection and adjuvant chemotherapy and radiotherapy have been the cornerstones of primary and secondary hepatobiliary tumours and pancreatic cancer treatment. However, options are limited for many patients. Less than 20% are resectable at diagnosis and not all patients are fit enough for an operation or effective chemotherapy regimens. There is, however, emerging evidence of a dose-response relationship, proving that escalated radiation doses are associated with improved local control as well as overall survival in borderline resectable (BRPC) or locally advanced pancreatic cancer (LAPC). Conventional radiotherapy delivers a comparatively homogenous radiation dose to the target volume. In contrast, SABR treatments combine advanced image guidance systems, accurate dose delivery and hypofractionated regimes. This is to facilitate a deliberate heterogeneous dose distribution across the target. This means the radiation tolerances of surrounding OARs are respected, while the tumour receives a higher, ablative radiation dose. A number of SABR studies have yielded good results in the treatment of large hepatobiliary tumours, with 1-year local control exceeding 90% and acceptable toxicity. Furthermore, delivering these hypofractionated ablative doses of radiation over a shorter treatment schedule has the potential to reduce the burden of treatment on patients.
However, with conventional SABR this therapeutic approach is often limited by concerns regarding organ motion and the possibility of developing small bowel radiation toxicity. As a result, many patients are only being treated with systemic agents. This is a prime example of where the elements of SMART on an MR-linac can facilitate an effective radiation dose escalation, while still respecting the radiation tolerance of normal tissues and surrounding OARs. In fact, using an MR-linac, it has been possible to successfully increase the prescribed dose in patients with primary pancreatic cancer. The previous standard dose was 33 Gy in five fractions, but SMART enables us to escalate the prescribed up to 40 Gy or even 50 Gy in five fractions. At the time of writing, 30 patients have been treated on the MR-linac for pancreatic tumours at GenesisCare.
Compassionate Access
The significance of MR-linac as an innovation in cancer treatment can’t be understated and, although at GenesisCare we are offering it in a private setting, we are committed to sharing the benefits of this technology with the wider medical community. Patients with localised pancreatic cancer have variable access to precision radiotherapy in the UK. The n-SARS-CoV-2 pandemic has further disadvantaged this patient group by reducing the availability and safety of surgery and chemotherapy. Considering this, since 2020 GenesisCare in association with GenesisCare Foundation, UK charity, Pancreatic Cancer Research Fund, ViewRay and University of Oxford have been treating NHS patients with localised pancreatic cancer with SMART at no cost. The programme, which is run through a partnership with the University of Oxford, is generating preliminary clinical and patient-reported outcome data on a UK cohort. This will inform the design of subsequent randomised clinical trials and help to embed SMART in UK oncology practice.
A new way of working
With any new technology, there comes a learning curve. MR-linac represents a significant change in working practices. It demands a style of inter-disciplinary working which challenges the norms.
In a standard radiotherapy workflow, a patient will receive a treatment planning CT one to two weeks before the start of treatment. During this time, several steps are carried out by a team of dosimetrists, physicists, doctors and radiographers to produce a treatment plan ready for the patient’s first fraction. These steps include contouring the treatment target and OARs and optimising the machine parameters to deliver the prescribed dose to the target while sparing critical structures. This is followed by reviewing the dose distribution, checking the planning process to ensure no errors have occurred and performing an independent dose calculation.
As part of the on-table adaptive workflow, the time taken for this process must be reduced from days to minutes. In order to achieve this, close inter-disciplinary working between the team is required. The need to undertake a number of complex tasks during each adaptive treatment also increases the time for each fraction to around one hour.
The MRIdian workflow involves a Clinical Oncologist on-site during treatment to oversee the daily adaption. To maintain a treatment schedule at GenesisCare, this has meant that clinicians had to be trained to contour all areas of anatomy, often working outside their main area of specialism. Equally challenging was the need to acquire skills in MRI interpretation, which for some specialities is not routinely used as a diagnostic modality. These were all skills that needed to be honed and validated before any patients could be treated on the MR-linac. In our case, we spent many hours learning with colleagues in MR-linac centres of excellence around the world. Twelve months later, we are experts in this field and have treated over 170 patients.
A body of evidence
There is a growing body of data as the global MR-linac community treats ever more and complex cases. We brought this international best practice to GenesisCare and have treated complex and challenging cases, including central lung, pancreas and reirradiation within our first year. We have many case studies available on our website genesiscare.com/mridian/case-studies. We already knew that the technology could deliver, but it was the confidence in our processes and the ability of our team to implement an adaptive workflow in a time-pressured environment, with a patient on the treatment table, which allowed us to embrace the opportunity that MR-linac presents in radiotherapy.
GenesisCare will install the second MR-linac in the UK in 2021. Through our MagNET programme, we are joining with NHS organisations to support education in the use of MR-guided radiotherapy. Enquiries to: James.Good@genesiscare.co.uk
Dr Ben George, Lead Physicist – MR Linac, GenesisCare
Ben is Lead Physicist – MR Linac at GenesisCare UK. He works as part of a multi-disciplinary team which has established a successful and world-leading SABR service delivering complex MR-guided adapted treatments. He has a PhD in Physics with a strong background in computer science, research and clinical computing. He has over ten years of experience as a Clinical Scientist specialising in radiotherapy in both the NHS and the private sector, and as a research scientist for the University of Oxford.
What do tiny bees and dead salmon have to do with the history of MRI? This post by Dr David Higgins and Dr Matthew Clemence explores how the flexibility of MRI lends itself to important applications outside of medicine and examines how the use of functional MRI has more recently brought us much closer to real scientific observation of the brain.
MRI is a rapidly evolving imaging modality, and the history of MRI has always been intertwined with research. Its flexibility lends itself to fascinating applications outside of medicine; even bees, and fish.
In neurobiology, honeybees are a common model for analysing underlying neural mechanisms because of their simply structured nervous system. By investigating the bee brain’s anatomy, correlations between anatomy and function can be studied. See Haddad et al 2004 for MR images of tiny bee brains. One early project looked to see if there were any magnetic structures inside the bee – which MRI was uniquely sensitive to – that might help bees navigate. Bees have been studied by MRI surprising often, perhaps because their behaviour is extraordinary, emerging as it does from such apparently simple creatures. MRI has helped our understanding of this important crop animal (Tomanek et al, 1996).
Looking at the function of intact, living neuroanatomy has been a dream for students of the human mind for centuries. Phrenology (from Ancient Greek φρήν (phrēn) “mind”, and λόγος (logos) “knowledge”), which supposed that the lumps and bumps on the skull reflected personality traits, was developed in 1796 and remained influential up until the 1840s. While, in a marked understatement from Wikipedia, “the methodological rigor of phrenology was doubtful even for the standards of its time”, the underlying concept that that the brain is the organ of the mind – and that certain brain areas have localised, specific functions – is based in fact. Technology developments in electroencephalography, near-infrared spectroscopy and most recently functional MRI have brought us much closer to real scientific observation of the brain.
Which brings us to a dead salmon…
Functional MRI (fMRI) was a revolutionary technique used to identify highly localised changes in blood flow resulting from differential load on regions of the brain. John (Jack) Belliveau at Massachusetts General Hospital showed in a key Science paper that these changes could be measured with MRI (Belliveau et al, 1991) in conjunction with a Gadolinium contrast agent, but it was Seiji Ogawa who demonstrated a practical, non-invasive method with the University of Minnesota (Ogawa et al, 1990). For the first time, scientists had access to detailed 3D anatomical images of the brain in action, through a safe technique that could be repeatedly used on volunteers. Its ease of use, combined with wide availability, allowed the technique to be adopted rapidly in psychology and neuroscience, often in the hands of the non-MRI specialist. Some of the early studies exploring this new ability to “read minds” often drew overly broad conclusions from badly designed experiments. This almost relegated fMRI into a category of “modern phrenology”.
The dead salmon experiment showed how, with naive experimental design and data analysis, fMRI could give convincing results on a dead Atlantic salmon (Bennett et al, 2010) and was a salutary lesson to would be fMRI researchers to improve their methodology (Lyon, 2017).
Now, once again fMRI is being used to tease out our inner thoughts, whether to attempt to detect lying for legal purposes or read letters directly from the visual cortex. This could have a dramatic impact in patients with “locked in syndrome” through the development of brain computer interfaces (Sorger, 2010).
fMRI has also found an unusual application in neuromarketing: the application of neuroimaging methods to product marketing, to more effectively “match products with people”. Companies can incorporate use of fMRI in the design process of a product, as well as in assessing the effectiveness of an advertising campaign, even if the “product” is a political candidate. “Political marketing is aimed at selling an existing candidate but, with more foresight, can also be used to “design” a better candidate” (Ariely & Berns, 2010). Imaging our brains may reveal what we really think (or how we’re likely to vote), even if we can’t fully articulate our preferences yet.
If all this sounds hard to believe, perhaps a look at our brain scans could help you decide whether to believe us. “The relative reduction in prefrontal grey matter relative to white may also predispose to a general antisocial disinhibited tendency which, coupled with increased white matter, results in excessive lying.” (Yang et al, 2005).
Just check the study passes the dead salmon test!
To see how Philips can help you in neuroscience visit:
Ariely D & Berns G. Neuromarketing: the hope and hype of neuroimaging in business. Nat Rev Neurosci 2010;11:284–292. doi:10.1038/nrn2795
Belliveau JW et al. Functional mapping of the human visual cortex by magnetic resonance imaging. Science 1991;254:716-719. doi:10.1126/science.1948051
Bennett et al 2009. Neural correlates of interspecies perspective taking in the post-mortem Atlantic salmon: An argument for proper multiple comparisons correction. J Serendipitous Unexpected Results 2010;1:1–5. See https://www.nature.com/articles/nj7420-437a
Haddad D et al. NMR imaging of the honeybee brain. J Insect Sci 2004;4:7. doi:10.1093/jis/4.1.7
Lyon L. Dead salmon and voodoo correlations: should we be sceptical about functional MRI? Brain 2017;140;e53. doi:10.1093/brain/awx180
Ogawa S et al. Brain magnetic resonance imaging with contrast dependent on blood oxygenation. Proc Natl Acad Sci U S A. 1990;87:9868-9872. doi:10.1073/pnas.87.24.9868
Sorger et al. A real-time fMRI-based spelling device immediately enabling robust motor-independent communication. Curr Biol 2012;22:1333-8. doi:10.1016/j.cub.2012.05.022
Tomanek B et al. Magnetic resonance microscopy of internal structure of drone and queen honey bees, Journal of Apicultural Research, 1996;35:3-9. doi:10.1080/00218839.1996.11100907
Wikipedia contributors. “Phrenology.” Wikipedia, accessed 16 Oct. 2020. Yang Y et al. Prefrontal white matter in pathological liars. Br J Psychiatry 2005;187:320-325. doi:10.1192/bjp.187.4.320
Dr David Higgins and Dr Matthew Clemence are Senior Scientists at Philips, part of the UK&I MR Clinical Science team and the wider global Philips Clinical Science group. They provide: MR physics support; advanced teaching on the functions of the MR system; prototype pulse sequence deployment and monitoring; novel pulse sequence development advice; guidance for novel image reconstruction and analysis projects; advice for novel interfacing novel hardware.