In the third blog of her series on AI and the radiographer, Shamie Kumar explores the impact on the radiographer when AI is integrated within an imaging modality.
In previous BIR blog posts, I have explored how AI is integrated into PACS with the AI outputs seen on radiology systems, and whether non-reporting radiographers could learn and benefit from AI. The question to explore in this blog is when AI is integrated within an imaging modality itself and how that may impact a radiographer.
AI embedded into a portable digital X-ray machine
Radiographic images are acquired in multiple modalities within different patient pathways. I will explore how AI embedded into a portable digital X-ray machine might change and affect how the radiographer works and learns.
Every radiographer is trained to take X-rays on portable machines and this is a core skill and it is an adapted technique compared with dedicated static X-rays rooms. It is unique in the sense patient positioning can vary depending on the environment and situation, whether this be on a ward or in A/E resus. Patient’s conscious level and mobility can vary, often supine and not all being cooperative. There can be situations where other healthcare professionals (HCP) are in proximity of the patient being imaged due to the image being acquired outside of the main radiology department.
AI output
Some hospitals have adopted digital portable X-ray machines to provide an instant image, the radiographer can see the chest X-ray immediately after exposure and decide whether the image quality is optimal. As AI becomes integrated within the modality, in this instance on a portable digital X-ray machine, the radiographer will also see the AI output and findings alongside the original X-ray. Not only does the radiographer see the AI output but other HCP that are present will also have the accessibility to view the same in the given environment. As we all know, X-rays need to be reported by radiologist or reporting radiographers, but often clinicians make clinical decision before these inpatient portable x-rays reports are finalised and available on the hospital system, especially if quick intervention is required.
When AI integration is done in such a way that radiographer need not log into PACs to view the AI output and is shown on the modality once the image is acquired, all radiographers can utilise AI to its full potential. The focus quickly shifts to: does the radiographer have the relevant education and training to understand the AI intended use, the AI outputs, what are the functions, features of the AI, how do they clinically interpret these images, how does AI work and what are the limitation of AI. All these questions become important when an AI is implemented; radiographers need to be trained how to use it, become familiar with the outputs, and educate others around them. If this is approached robustly, it will empower radiographers to learn and upskill themselves with AI being part of their daily clinical workflow, giving them the confidence to support and guide other healthcare professionals (HCPs) who also are looking at the X-ray when it acquired.
AI is an assistive tool
It’s important to recognize that AI findings are never the final diagnoses. Ultimately AI is an assistive tool, embedded within portable machines. Doctors and HCPs will also view the AI output and, with time, it will be the role of the radiographers to appropriately manage and guide other healthcare professionals.
About Shamie Kumar
Shamie Kumar is a practicing HCPC Diagnostic Radiographer; graduated from City University London with a BSc Honors in Diagnostic Radiography in 2009 and is a part of Society of Radiographers with over 12 years of clinical knowledge and skills within all aspects of radiography.
She studied further in leadership, management, and counselling with a keen interest in artificial intelligence in radiology.
Following the recent BIR live event Imaging explosion across the pond – causes and solutions in which the UK and USA radiology and healthcare systems were compared, DMC Radiology Reporting co-director Professor Simon Padley reflects on the UK position.
The USA often provides a window into our own future
In the application of imaging technology, we often follow trends that emerge in the US – the rise in CT and MRI utilisation are two examples, and more recently the growth of outsourcing is following a similar trajectory.
With different healthcare models, the US does not rely on central funding to replace or add to CT and MRI capacity. NHS funding comes from the government’s general revenue, and healthcare services are provided to all residents of the UK, regardless of their ability to pay. In contrast, the US medical system is a mixed system of public and private funding. It includes a combination of private health insurance, employer-based insurance, individual out-of-pocket payments, and public programs like Medicare and Medicaid, which are funded through federal and state taxes.
In 2022 there were 6.6 million CT studies on NHS funded patients according to NHS Digital, at a time when the population was reported to be 55 million. This equates to 121 studies per 1000 of the population. In the USA this figure is more than double at 278 CT studies per 1000 of the population (84 million CT studies in a population of about 333 million CT Scans Each Year – iData Research).
And that is just CT! Official data for 2021/22 shows that between April 2021 and March 2022, NHS services in England carried out 43.8 million imaging tests across all modalities Ref. This reflects an ever-growing requirement for imaging studies to be undertaken and reported.
At the same time, the workforce needed for this activity has fallen far behind that required. We bump along the bottom of the league table for radiologists per 100,000 of the population (8.5). Europe has 13, the US 11. Couple this with complexities of pension taxation, IR35 and COVID related burnout all nudging older highly skilled and efficient radiologists towards the exit door and we have a perfect storm. Even today we have 2000 full-time consultant clinical radiologist posts unfilled across the UK. The RCR predicts a 39% workforce shortfall by 2026 (equating to 3166 full time radiologists).
This may create stress in the radiology department, but rest assured it also causes grey hair and sleepless nights for those that inhabit the carpeted management corridors. Hidden amongst every backlog of reporting there is serious pathology lying undiagnosed. When that report is provided, and the treatment options are discussed, some options will have closed, tumours will have stage shifted and outcomes will be less good. This constitutes a chief executive’s nightmare but has caught the medicolegal world’s attention. So, what are we to do?
Teleradiology and the NHS
Almost all acute trusts have turned to the services of the teleradiology community, now playing a vital role in helping to address this capacity shortfall. In the past 10 years the market has grown with a compound annual growth rate of about 10-15%.
Who are all these extra radiologists and where do they come from? Well of course, by-and-large, they are you and me. But we are a limited pool, the market rates for reporting (set by the NHS) are not great and there are only so many hours in the day.
So where can we look for additional workforce capacity and will we be allowed to access it? To allow this to happen the NHS will need to engage more readily with the solutions that are now emerging and examine the detail of how we, in the teleradiology world, are already addressing data governance and medicolegal concerns.
At DMC Radiology Reporting, we already work in partnership with many NHS Trusts. We strive to deliver fast, accurate radiology reporting with innovation and efficiency. We have a rigorous commitment to clinical governance, and we are proud of our work force of GMC-registered/FRCR-radiologists with sub-specialty interests. Like many others, we are interested in how these problems are being addressed in the US.
About Professor Simon Padley
In 2013 Simon co-founded DMC-Radiology Reporting, which has been growing and developing ever since, focusing on sub-specialist high quality outsourced reporting.
Simon is a cardiothoracic and interventional radiologist, appointed in 1994. As a previous imaging director in the NHS for many years he developed a range of new services, most recently as lead radiologist for Royal Brompton Hospital Diagnostic Imaging Centre, opened in 2022. This facility incorporates one of the only combined interventional bronchoscopy and radiology facilities in the country.
As a Professor of Practice (Diagnostic and Interventional Radiology) since 2016, at the National Heart & Lung Institute, Imperial College London, he maintains an active academic career, publishing widely with over 220 articles in peer reviewed journals.
Shamie Kumar describes how AI fits into a radiology clinical workflow and her perspective on how a clinical radiographer could use this to learn from and enhance their skills.
AI in radiology and workflow
We all know that AI is already here, actively being implemented and used in many trusts in seeing its real world value supporting radiology departments to solve current challenges.
Often this is focused on benefits to radiologist, clinicians, reporting radiographers, patients, and cost savings, but what about clinical non-reporting radiographers undertaking the X-ray or scans – can AI benefit them too?
Let’s think about how AI is implemented and where are the AI outputs displayed?
If the AI findings are seen in PACS, how many radiographers actually log into PACS after taking a scan or X-ray? Good practice is seen to have PACS open to cross-check images that have been sent from the modality. Often this doesn’t happen for various reasons but maybe it should be a part of the radiographers’ routine practice, just like post-documentation is.
Can Radiographers Up-Skill?
Given the view it does happen, radiographers will have the opportunity to look at the AI outputs and potentially take away learnings on whether the AI found something that they didn’t see initially or whether there was a very subtle finding. We all know people learn through experience, exposure, and repetition, so if the AI is consistently picking up true findings, then the radiographer can learn from it too.
But what about when AI is incorrect – could it fool a radiographer, or will it empower them to research and understand the error in more detail?
As with many things in life, nothing is 100% and this includes AI in terms of false positive and false negatives. The radiographers have the opportunity to research erroneous findings in more detail to enhance their learning, but do they actually have time to undertake additional learning and steps to interpret AI?
CPD, self-reflection, learning through clinical practice are all key aspects of maintaining your registration, and self-motivation is often key to furthering yourself and your career. The question remains: are radiographers engaged and self-motivated to be part of the AI revolution and use it to their professional benefit with potential learnings at their fingertips?
There have been a few recent publications that share insight on how AI is perceived by radiographers, what is their understanding, training and educational needs.
Many Universities like City University London and AI companies like Qure.ai are taking the initial steps in understanding this better and taking active efforts in filling the knowledge gap, training and understanding of AI in radiology.
Radiographers who are key part of any radiology pathway, are yet to see the real-world evidence on whether AI can upskill radiographers, but there is no doubt this will unfold with time.
About Shamie Kumar
Shamie Kumar
Shamie Kumar is a practicing HCPC Diagnostic Radiographer; graduated from City University London with a BSc Honors in Diagnostic Radiography in 2009 and is a part of Society of Radiographers with over 12 years of clinical knowledge and skills within all aspects of radiography. She studied further in leadership, management, and counselling with a keen interest in artificial intelligence in radiology.
References
Akudjedu, T. K. K. N. M., 2022. Knowledge, perceptions, and expectations of Artificial intelligence in radiography practice: A global radiography workforce survey. Journal of Medical Imaging and Radiation Sciences.
Coakley, Y. M. E. C. M. M., 2022. Radiographers’ knowledge, attitudes and expectations of artificial intelligence in medical imaging. Radiography International Journal of Diagnostic Imaging and Radiation Therapy, 28(4), pp. P943-948.
Malamateniou, K. P. W. H., 2021. Artificial intelligence in radiography: Where are we now and what does the future hold?. Radiography International Journal of Diagnostic Imaging and Radiation Therapy, 27(1), pp. 58-62.
Cheryl Cruwys, European Education Coordinator at DenseBreast-info.org/Europe, highlights the importance of understanding the screening and risk implications of dense breast tissue. DenseBreast-info.org’s mission is to advance breast density education and address the gap in knowledge about dense breasts.
Mammography remains the standard of care in screening for breast cancer and has been proven to reduce the mortality rate [1]. However, in dense breasts, cancers can be hidden/obscured on mammography [2,3] (Fig.1) and may go undetected until they are larger and more likely to present with clinical symptoms [4]. Breast density has also been identified as the most prevalent risk factor for developing breast cancer [5].
Women with dense breasts are BOTH more likely to develop breast cancer and more likely to have that cancer missed on a mammogram [5]
Fig. 1 – Cancer on a mammogram of a fatty vs a dense breast
What is Dense Breast Tissue?
Breasts are made of fat and glandular tissue, held together by fibrous tissue. The more glandular and fibrous tissue present, the “denser” the breast. Breast density has nothing to do with the way breasts look or feel. Whilst dense breasts are normal and common, dense breast tissue makes it more difficult for radiologists to detect cancer on a mammogram.
Breast density is determined through a mammogram and described as one of four categories (Fig. 2), (A) Fatty, (B) Scattered, (C) Heterogeneously Dense, (D) Extremely Dense. Breasts that are (C) heterogeneously dense, or (D) extremely dense are considered “dense breasts”. Fig. 2
Figure 2
Dense Breasts Facts
40% of women over age 40 have dense breasts.
Dense breast tissue is an independent risk factor for the development of breast cancer; the denser the breast, the higher the risk.
Mammograms will miss about 40% of cancers in women with extremely dense breasts.
Women with extremely dense breasts face an increased risk of late diagnosis of breast cancer.
In these women, screening tests, such as ultrasound or MRI, when added to mammography, substantially increase the detection of early-stage breast cancer.
Dense Breast Educational Resources
DenseBreast-info.org/Europe is the world’s leading website about dense breasts. This medically-sourced resource is the collaborative effort of world-renowned experts in breast imaging and medical reviewers. Fig 3.
Figure 3
The website features educational tools for both European Patients and Providers Fig. 4. (a and b)
Figure 4 (a)
CME Course – Learn Why Breast Density Matters!
The DenseBreast-info.org resource includes a free CME/CE course, Dense Breasts and Supplemental Screening suitable for primary care healthcare providers, including family medicine, internal medicine, and OB/GYN physicians and midlevel providers, as well as radiologists, and radiologic technologists (UEMS-EACCME® mutual recognition for AMA credits).
A growing number of medical organisations link to the DenseBreast-info.org website, including the EFRS (European Federation of Radiographer Societies) and the Society of Radiographers.
Figure 4 (b)
The website includes breast screening guidelines in Europe. A comparative analysis table summarises the guidelines in each country.
NHS Breast Screening Programme
Currently in the UK, population routine screening mammograms are offered to women aged 50–74, every 3 years. Though dense breasts affect the likelihood that a cancer will be masked and increases a woman’s risk for developing breast cancer, it is not part of UK data collection. A woman’s breast density is not assessed, not recorded in medical records, nor reported to her. For diagnostic purposes, this may differ. However, in many other European country screening programs, a woman’s breast density is assessed, recorded, and the woman’s personal breast density category is included in the mammography report.
News in Europe: the EUSOBI Recommendations
Population based breast screening guidelines vary across Europe. In the UK, asymptomatic women attending routine national breast screenings receive mammography alone. In some countries (e.g., Austria, Croatia, Hungary, France, Serbia, Spain, Switzerland) screening guidelines for women with dense breasts include that they be offered supplement ultrasound following a mammogram.
Following recent MRI screening trials there is cumulating evidence which confirms that women with dense breasts are underserved by screening with mammography alone [7,8]. In March 2022, new guidelines were issued in Breast cancer screening in women with extremely dense breasts by the European Society of Breast Imaging (EUSOBI) [9] highlighting the growing evidence, particularly the results of a randomised, multicentre controlled study, the Dense Tissue and Early Breast Neoplasm Screening (DENSE) Trial. [7,8]
The European Society of Breast Imaging 2022 recommendations now step away from the one-size-fits all approach of mammography that is currently adopted by most European screening organizations and advocates for tailored screening programmes. There is compelling evidence that the new recommendations enable an important reduction in breast cancer mortality for these women.
Summary of the EUSOBI Recommendations
Below is EUSOBI’s summary graphic of the recommendations (Fig. 7) that highlight:
Supplemental screening is recommended for women with extremely dense breasts.
Supplemental screening should be done preferably with MRI …. where MRI is unavailable… ultrasound in combination with mammograph may be used as an alternative.
In addition to recommended additional screening in women with extremely dense breasts, note that EUSOBI recommends that“women should be appropriately informed about their individual breast densityin order to help them make well-balanced choices.”
EUSOBI acknowledges that it may take time before the new recommendations are implemented in Europe and that the level of implementation is dependent on the resources that are available locally.
It is important to emphasize that the EUSOBI recommendations highlighted in this article are not yet guidelines in Europe. Of course, it is hoped that in Europe, national breast screening committees try to implement these recommendations as soon as possible to benefit women.
Figure 7
World Dense Breast Day Success!
DenseBreast-info.org launched the first #WorldDenseBreastDay on 28 September 2022.
Nearly 100 posts with great images were created and ran for 24 hours across social media channels. Analytics detailed participation from people in 37 countries, over 8.6 million people saw/read the posts and over 17,000 people interacted with the posts.
The purpose of the day is to raise awareness about dense breasts and share medically-sourced educational resources available for women and health providers.
Please join us next year for #WorldDenseBreastDay which will take place on 27 September 2023!
Take Home Message:
Breast density can both hide cancers on a mammogram and increases the risk of developing breast cancer.
Women with dense breasts benefit from additional screening tests after their mammogram
Breast density education and access to supplemental screening can mean the difference between early- or late-stage diagnosis
Physicians should be educated and prepared to have patient conversations about breast density
1, Tabar L, Vitak B, Chen T H et al. Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology 2011;260:658-63
2. Hooley RJ, Greenberg KL, Stackhouse RM, Geisel JL, Butler RS, Philpotts LE (2012) Screening US in patients with mammographically dense breasts: initial experience with Connecticut Public Act 09-41. Radiology 265:59–69
3. Kolb TM, Lichy J, Newhouse JH (2002) Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology 225:165–175
4. RoubidouxMA, Bailey JE,Wray LA, HelvieMA(2004) Invasive cancers detected after breast cancer screening yielded a negative result: relationship of mammographic density to tumor prognostic factors. Radiology 230:42–48
5. McCormack VA, dos Santos Silva I (2006) Breast density and parenchymal patterns as markers of breast cancer risk: a metaanalysis. Cancer Epidemiol Biomarkers Prev 15:1159–1169
6. Vourtsis A, Berg W A. Breast density implications and supplemental screening. Eur Radiol 2019;29:1762-77.
7. Bakker M F, de Lange S V, Pijnappel R M et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med 2019;381:2091-102.
9. Mann, R.M., Athanasiou, A., Baltzer, P.A.T. et al. (2022) Breast cancer screening in women with extremely dense breasts recommendations of the European Society of Breast Imaging (EUSOBI) Eur Radiol 32, 4036–4045
Cheryl Cruwys is a British breast cancer patient, advocate, author and educator. While living in France (2016) she was diagnosed with early-stage breast cancer and credits the early detection of breast cancer to the French standard practice of performing supplemental screening on dense breast tissue. She is founder of Breast Density Matters UK, European Education Coordinator at DenseBreast-info.org/Europe, a member of the European Society of Radiology Patient Advisory Group and a Patient Rep on the ecancer.org Editorial Board.
Cheryl works at the European level with patient advocacy and medical societies, attends/presents at key scientific symposiums and works with international breast imaging experts to disseminate education on dense breasts. DenseBreast-info.org
We are all familiar with the concept of artificial intelligence in radiology and its application that is expanding rapidly. But how will AI in the workplace affect the radiographer and how does it differ from the red dot system radiographers are so familiar with?
Shamie Kumar describes her perspective on how radiography has evolved over time, the impact radiographers can have in detecting abnormal X-rays and reflects how she views fast approaching AI in advancing current skills.
The Red Dot System
Often one of the first courses a newly qualified radiographer attends is the red dot course. This course demonstrates pathologies and abnormalities often seen in X-rays some obvious, others not, giving radiographers the confidence to alert the referring clinician and/or radiologist that there is something abnormal they have seen.
The red dot system is a human alert system, often two pairs of eyes are better than one and assist with near misses. How this is done in practice can vary between hospitals, in the era of films the radiographer would place a red dot sticker on the film itself before returning it to clinician or radiologist. In the world of digital imaging this is often done during “post documentation” a term used once the X-ray is finished, the radiographer will complete the rest of the patient documentation to suggest the X-ray is complete, ready to be viewed and reported. As part of this process the radiographer can change the status of the patient to urgent along with a note for what has been observed. From this the radiologist knows the radiographer has seen something urgent on the image and the patient appears at the top of their worklist for reporting and, so the radiologist can view the radiographer’s notes.
The Role of AI in Radiology
Artificial Intelligence (AI) is moving at a pace within healthcare and fast approaching radiology departments, with algorithms showing significant image recognition in detecting, characterisation and monitoring of various diseases within radiology. AI excels in automatically recognising complex patterns in imaging data providing quantitative assessments of radiological characteristics. With the numbers for diagnostic imaging requests forever increasing, many AI companies are focusing on how to ease this burden and supporting healthcare professionals.
AI triage is done by the algorithm based on abnormal and normal findings. This is used to create an alert for the referring clinician/radiologist. It can be customised to the radiologist, for example colour-coded flags, red for abnormal, green for normal, patients with a red flag would appear at the top of the radiologist worklist. For the referring clinicians who don’t have access to the reporting worklist, the triage would be viewed on the image itself with an additional text note suggesting abnormal or normal.
Image courtesy of qure.ai
What does AI do that a radiographer doesn’t already? AI is structured in a way that it gives the findings; for example, a pre-populated report with its findings or an impression summary and its consistent without reader variability. So, the question now becomes what can AI do beyond the red dot system. Here, the explanation is straightforward. Often a radiographer wouldn’t go to the extent of trying to name what they have seen, especially in more complex X-rays like the chest where there are multiple structures and pathologies. For example, a radiographer would mention right lower lobe and may not go beyond this, often due to confidence and level of experience.
AI can fill this gap; it can empower radiographers and other healthcare professionals with its classification of pathologies identifying exactly what has been identified on the image, based on research and training of billions of data sets with high accuracy.
The radiographers may have the upper hand with reading the clinical indication on the request form and seeing the patient physically, which undoubtably is of significant value. However, the red dot system has many variables specific to that individual radiographer’s skills and understanding. It is also limited to giving details of what they have noted to just the radiologist. What about the referring clinician who doesn’t have access to the radiology information system (RIS) where the alert and notes are? Do some radiographers add a text note on the X-ray itself?
Summary
Yes, AI is a technological advancement of the red dot system and will continue to evolve. It is structured in how it gives the findings and does this consistently with confidence adding value to early intervention, accurate patient diagnosis, contributing to reducing misdiagnosis and near misses. AI is empowering radiographers, radiologists, referring clinicians and junior doctors by enhancing and leveraging their current knowledge to a level where there are consistent alerts and classified findings that can even be learned from. This doesn’t replace the red dot system but indeed enhances it.
The unique value a radiographer adds to the patient care, experience and physical interaction can easily be supplemented with AI, allowing them to alert with confidence and manage patients, focusing the clinician time more effectively.
About Shamie Kumar
Shamie Kumar is a practicing HCPC Diagnostic Radiographer; graduating from City University London, BSc Honors in Diagnostic Radiography in 2009 and part of Society of Radiographers with over 10 years of clinical knowledge and skills within all aspects of radiography. She studied further in leadership, management and counselling with a keen interest in artificial intelligence in radiology.
Time is everything when it comes to breast cancer care. If we can embrace smarter technology, this will help to provide better workflow efficiency and clinical confidence across the patient pathway, unlocking that much needed time to care for breast cancer patients. Tim Simpson General manager, UK and Ireland at Hologic explores how we can achieve this across the breast health continuum of care.
More accurate and efficient detection is instrumental for better patient outcomes. 3D Mammography™ systems have become smarter, bringing breast cancer diagnosis to a new level, improving cancer detection accuracy, optimising workflow, and supporting personalised patient care[1]. The integrated AI powered software solutions employ machine-learning and deep learning algorithms developed and trained on a large number of tomosynthesis (3D Mammography™) images to aid cancer detection, assess breast density, and accelerate diagnosis.
What’s more, using 3D Mammography™ can result in up to 40% fewer recalls[2], [3], helping to reduce the physical and emotional burden on patients and giving back valuable time to health care professionals.
To mitigate the time challenges typically faced when reporting tomosynthesis images, advanced imaging technology can reconstruct high-resolution tomosynthesis slices which results in a reduction in radiologist reading time.
More efficient detection can also be achieved when performing a contrast mammography examination. It’s possible to combine the power of Contrast Enhanced Mammography (CEM) with 2D and tomosynthesis images all in one compression to provide anatomical and functional imaging in a singular exam. The use of comprehensive imaging using co-registered functional and morphological information can reduce reading time to seven – ten minutes versus thirty to sixty minutes for a standard breast MRI[4],[5].
Almost 43% of women over 40 years old have dense breast tissue that can obscure lesions on traditional 2D mammograms, making cancers harder to detect and recalls more likely[6]. Women with very dense breasts have a four to five times greater risk of developing breast cancer in comparison to women with less dense breasts[7].
This is where new AI–powered technologies have the potential to help identify women who are particularly at high risk of breast cancer, specifically those women with extremely dense breasts.
Assessing women using automated breast density analysis software is a simple way to ensure that those most at risk of developing breast cancer are prioritised for screening, on potentially a more regular basis, whilst the screening interval for those women at lower risk could be extended, creating a more efficient and personalised breast screening program in the longer term.
Diagnostic innovation is on a trajectory that we cannot ignore. It is evident that AI is sure to revolutionise healthcare. There will be multiple benefits associated with the adoption of AI technology in breast imaging for patients and clinicians alike; for example, enhanced clinical confidence, improved workflow efficiencies, accelerated disease detection and increased accuracy of breast cancer diagnosis. Hologic is proud to be leading the way with its AI solutions for our customers and partners, helping to save time and lives across the breast health continuum of care.
1 Philpotts L, Kalra V, Crenshaw J, Butler R ‐ Radiological Society of North America 2013, SSK01‐09
[2] Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014 Jun 25;311(24):2499-507.
[3] Olivia DiPrete, Ana P. Lourenco , Grayson L. Baird, Martha B. Nov 2017. Mainiero. Screening Digital Mammography Recall Rate: Does It Change with Digital Breast Tomosynthesis Experience?. Radiology: Volume 286: Number 3—March 2018
[5] Julie Sogani,a Victoria L. Mango,a Delia Keating,a Janice S. Sung,a and Maxine S. Jochelson. Contrast-Enhanced Mammography: Past, Present, and Future. Clin Imaging. 2021 Jan; 69: 269–279.
[6] Sprague BL, Gangnon RE, Burt V, et al. Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst. 106(10), 2014.
[7] Ingrid Schreer. Dense Breast Tissue as an Important Risk Factor for Breast Cancer and Implications for Early Detection. Breast Care (Basel). 2009 May; 4(2): 89–92.
Steve Holloway, from Signify Research explores the daunting challenge of navigating the road to Enterprise Imaging.
Cloud technology is transforming how we live and work today. For healthcare providers undergoing long-term digitalisation, the potential of cloud technology resonates, yet the complexities of adoption are daunting and difficult to navigate. Nowhere is this more evident in healthcare than imaging informatics.
A front-runner of healthcare digital innovation, the imaging sector has a complex legacy of on-premise, siloed, best-of-breed applications that interact with and influence every point of the care continuum.
Many providers have taken the positive steps of embarking on an enterprise imaging strategy, federating imaging service line applications, centralising data management and transforming access for diagnosticians, care givers, and patients.
Progress on this mission has been challenging however, in part due to an over-reliance on aging on-premise applications and limited availability of alternatives.
Today, a new generation of cloud-based enterprise imaging solutions is emerging, offering a tangible route to cloud. In this paper, we’ll identify the key characteristics of this new generation of cloud-based products and outline the key drivers and barriers to their adoption.
Further, we’ll describe the long-term transformative power that cloud offers for enterprise imaging and the future of healthcare provision, providing our view on the key considerations for providers navigating cloud adoption for enterprise imaging.
Dr Gareth Davies describes the massive impact the COVID 19 pandemic had on elective cross-sectional reporting, reducing output to almost zero. Here he reflects on how the drive for innovation and the motivation to think differently led to a better teleradiology service for both patients and staff.
Dr Gareth Davies
The pandemic will certainly define us as an organisation. A period of uncertainty, business survival, the protection of our staff and their livelihoods and a readiness to provide a clinical service our patients rely on.
Let’s go back to the 1 January 2020. It was a time when the UK’s radiology reporting capacity was at a tipping point, backlogs of unreported examinations were in the thousands, demand for imaging services was constantly increasing, and more and more patients were being scanned. Just in one single day in that month, Telemedicine Clinic (TMC) reported over 1400 elective cross-sectional scans to its NHS customer base.
Wind the clock forward to May 2020, and during the midst of the Coronavirus pandemic a grand total of 11 plain films were reported in a whole week.
TMC’s business is teleradiology, a service that underpins delivery of clinical services to the customers it reports for. Take away the need for outsourcing by having to stop elective scanning and there is no need for teleradiology. Take away elective scanning and the backlogs built up over time can be cleared. The reset button had been pressed and no one knew what was going to happen next.
TMC employ over 300 radiologists, with over 50 radiologists working in the emergency section. The recovery for this section was quick with demand returning to normal volumes after 3 months. The recovery of the elective service has stalled in line with countrywide lockdowns but is now about 60% and getting busier.
So how did a company that had 50% of its business disappear overnight survive? The simple answer was innovation!
Response team
The first thing TMC did was to call on its European based radiologists, staff, and management teams to team up to provide an unrivalled knowledge-share hub. Coronavirus imaging from hospitals all over the world was collated to provide real-time COVID reporting best practice as the world started to understand the virus more. In addition, top thoracic specialist radiologists from Europe who had already experienced COVID radiology were called to report cases for NHS hospitals. A new “24/7 COVID response” reporting team was established in less than 2 weeks.
On the back of our experience with the 24/7 COVID Response service, the TMC Academy used our reporting experience and best practice from other nations experience to create two COVID-19 online reporting modules on the TMC Academy platform and made these free to all to view and learn from.
Platform
Our next step was the deployment of the TMC Platform for our NHS customers. Where TMC had a contract in place with a Trust who also had reporting radiologists collaborating with TMC, TMC enabled the radiologist to work for their hospital using the TMC infrastructure and IT, free of charge such that the radiologist could work remotely reporting their cases, where home reporting was not available at that time. Driving down costs to our customers in the future is a focus of TMC.
TMC is proud of its recruitment process for radiologists. Our traditional model was to invite potential colleagues to our head office in Barcelona, to undergo a series of interviews and undertake test case examinations specific to their subspecialty. What do you do when you need to recruit radiologists in a period of complete lockdown, with the inability to travel even a few miles? You challenge your teams to virtualise a 3-week induction/test period of course! This was completed again using the online TMC Academy platform to make sure all radiologists were fully vetted, interviewed, examined and quality-assured to comply with our standards and strict working regulations required to support the UK market and the NHS.
Hub
Prior to the pandemic, TMC were aware of a growing need for acute reporting services ranging from neuro MRI ad hoc reporting to Emergency CT daytime cover to sub-specialist short turn around reporting. One of our major ambitions during this period was to innovate more integrated clinical care and break the traditional concept of teleradiology and the clearing of backlogs and night time on call. TMC are good at elective reporting and using UK and European based radiologists. TMC are also good at UK overnight Emergency CT reporting from wide awake UK and European radiologists who have moved to Australia. However, there is a mix of requirements that TMC did not fully cater for and the NHS desperately requires. From conversations with customers, it was clear that elective reporting, although destined to return with a vengeance, was not the priority. The main driver in fact was a mixture of acute and semi-urgent work so, from this, The TMC Hub and TMC Oncology concepts were created.
Any time of the day or night, a clinician, radiographer, or radiology manager can call TMC to discuss scanning a patient. These can be emergency patients in the day or night, they can be acute inpatients who simply need that next step in their pathway or to be discharged safely, or perhaps just a routine scan which feels urgent. The TMC Hub can help put the patient on the right pathway for their care, anytime day or night, Monday to Friday or a weekend. TMC’s customers love the new HUB concept, it provides a real safety net that they can contact us to get a patient scan completed, all within the hospitals set guidelines.
Artificial Intelligence
Last but not least, during the pandemic, TMC has had the opportunity to establish a dedicated team to evaluate the plethora of AI products on the market and implement products which we believe will improve patient care. Through stringent evaluation, TMC now has a number of AI products in place to assist its radiologists in making a clinical report. For the emergency section, AI now looks at all CT PA examinations for pulmonary embolism (PE), subtle C-spine fractures in trauma scans and intracranial haemorrhage in CT brains. For elective services, the AI software looks for PEs in all CT examinations that involve the thorax as soon as the examination arrives in the TMC PACS. In our new low dose CT thorax reporting for the NHS lung screening / lung health check service, we are using nodule detection and automated reporting to the requirements of the NHS QA standards for such a service. And new to TMC’s repertoire is a novel service, bringing AI to its clients without them knowing it. Through TMC’s IT infrastructure, our AI solution can look at ALL images in a customers PACS to identify incidental PEs, assign them to a TMC radiologist for immediate reporting which is flagged to the clinician team on-site in real-time. A scan that could have waited 3 weeks for reporting with unknown downstream costs to the Trust. AI will not replace radiologists, but it will improve radiology workflows, something which TMC can help clients do.
Benefits
With innovation comes benefit, a benefit that can be passed on to our customers in terms of reduced costs for delivery as well as reduced costs further down the patient pathway. Innovative services such as the TMC Hub or the TMC Oncology service will give clients the confidence they need to get a scan reported first time by the most appropriate and qualified radiologists.
Teleradiology and outsourced radiology are looked upon as a cost to the NHS which needs to be removed. With over 90% of NHS services relying on overnight emergency services being delivered from the independent sector, it is hard to see how this will change any time soon. Instead, looking at how teleradiology can help underpin service delivery, provide the AI analysis and expertise, provide the IT network to telework over international borders whilst using capacity from Europe to add to the overstretched UK workforce, the question should be how can we integrate more with our providers to deliver value-driven innovative healthcare to all people.
About Gareth Davies
Dr Gareth Davies, UK Medical Director Head and Body Section (Full time employed) Dr Davies has 18 years’ experience as a Consultant Radiologist in the South Wales NHS prior to joining TMC in 2019. He has a specialist interest in interventional and oncological radiology and held various national roles including the Regional Specialty advisor for training in Wales (Royal College of Radiologists), a member of the Clinical Radiology Specialty Training committee (RCR), Lead Radiologist and Lead QA of the Wales Abdominal Aortic Aneurysm Screening Programme (WAAASP), Associate Medical Director of Cancer Diagnostics and the Clinical Lead of the Early Cancer Diagnosis Programme, Wales Cancer Network and member of the Clinical Advisory Panel for CRUK. Since Joining TMC, Dr Davies has been involved in helping form TMC Oncology as well as working within the UK Business Unit to develop a more clinically integrated approach to telemedicine with the NHS forming the TMC Hub concept.
One of the first doctors to use radiology to diagnose diseases of the nervous system, Artur Schüller began his first systematic survey of the skull just a few years after X-rays were first discovered. Here, Andrew Schuller, a distant cousin, describes his extraordinary academic and personal journey which led to his recognition as the “Father of Neuroradiology”.
Artur Schüller (hereafter Arthur Schuller) was born in the Moravian city of Brunn (now Brno in the Czech Republic) in 1874. Most of the Schullers in Brunn were involved in the textile industry but Arthur’s father, Jonas, was an ENT specialist. Arthur did well at the German-language secondary school and went on to enrol in the medical school of the University of Vienna, which at that time had an excellent international reputation. He graduated in 1899 sub auspiciis Imperatoris, a rare title only awarded by the Emperor to students who had scored perfect marks in all their school and university exams. This entitled him to select his post-graduate mentors and Arthur chose Wagner-Jauregg and Kraft-Ebbing, a combination that matched his interest in both anatomy and psychiatry. They sent him off to Berlin for 6 months in 1901 where he worked with Munk, Oppenheim and Krause who taught him about experimental physiology, clinical neurology and the diagnosis and treatment of brain tumours. By the time Schuller returned to work at the Allgemeine Krankenhaus, Vienna had already taken up Roentgen’s 1896 discovery of X-rays and Arthur was soon working with Guido Holzknecht, leader of Vienna’s radiological research efforts.
Arthur Schuller
Schuller was the first to describe the role of X-ray in diagnosing diseases of the nervous system. Working with dried skulls from the museum and with live patients his painstaking analysis of countless X-rays enabled him to produce the first systematic survey of the radiology of the skull, which described both normal and pathologic anatomy. This book The Skull base on the Radiogram (Die Schädelbasis im Röntgenbilde: Archiv und Atlas der Normalen und Pathologische Anatomie) was published in 1905 and was followed in 1912 by Röntgen-Diagnostik der Erkrankungen des Kopfes (Röntgen Diagnosis of Diseases of the Head) which encapsulated his extensive work on a range of topics and was eventually translated and published in 1918 by C V Mosby in America under the auspices of the US Army (Incidentally, during WW2 Schuller, by that time in Australia, wrote about battlefield head injuries and worked in a military rehabilitation hospital).
Schuller’s interests ranged widely. From 1904 he was Director of the Children’s Hospital where he had worked in both the Neurology and the Psychiatric Clinics. But he maintained his experimental lab work and practice at the Allgemeine Krankenhaus. By 1907 he not only passed his Habilitation (PhD) but was also awarded Dozent status which allowed him to teach courses at the university as well as privately; he kept an X-ray machine in his home. When he was made a University Professor in 1914 he was the youngest in the medical faculty. In addition to his contributions to neurosurgical procedures (transsphenoidal approach to the pituitary, antero-cordotomy and hydrocephalic drainage) Schüller is associated with three bone diseases: the Hand Schüller Christian syndrome, osteoporosis circumscripta and cephalohaematoma deformans. But it is in his foundational work in forming the discipline of Neuroradiology that his outstanding contribution lies.
The financial stringencies and the political volatility that followed the collapse of the Austro-Hungarian Empire in 1918 had a serious impact on the ability of the Vienna Medical School to maintain its position at the forefront of medical research. But the continuing presence of so many prominent medical scientists enabled it to retain its international reputation. Along with Wagner-Jauregg Schuller was instrumental in expanding the existing post-graduate courses which attracted students from round the world. The US even established The American Medical Society of Vienna to administer the flow of almost 12,000 American students who enrolled in these courses between 1921 and 1938. Schuller continued to write papers and teach but he also consolidated his international reputation by travelling the world to lecture at conferences and clinics in the UK, Europe, Latin America and the US, where he lectured at the universities of Chicago, Johns Hopkins and New York and the Mayo clinic. In teaching and travelling he established strong personal contacts that would stand him in good stead including both Harvey Cushing and Walter Dandy in the US, both pioneering neurosurgeons with an interest in radiology. In 1935, while attending the Second International Neurological Congress in London, he met Hugh Cairns, an Australian neurosurgeon, who invited him to come to Oxford. Perhaps the apex of Schuller’s career was the central role he played in the first international congress of neuroradiologists. This, the First Symposium Neuroradiologicum was held in Antwerp in July 1939; the 22nd symposium will be held in 2022. There are some who assert that it was the Swede Lysholm who really established neuroradiology by developing contrast radiography, though it was Dandy who first wrote about ventriculography.
Schuller may not have pursued contrast radiography because of the lack of research facilities in interwar Vienna or because of the eclecticism and breadth of his intellectual interests but there is no doubt that his work was foundational for the routine radiography of the sella and its environs and the diagnosis of pituitary tumours. At the eighth Symposium Neuroradiologium in 1967 Bull and Fischgold declared “Without a shadow of doubt Arthur Schuller was the father of neuroradiology”. Schuller’s papers are still quoted in current literature and the Austrian Neuroradiological Society awards and annual Arthur Schüller Prize.
The Antwerp Symposium 1939
Schuller’s private life also flourished. In 1906 he had married Margarete Stiassni from a family of successful textile industrialists in Brunn. Arthur and Margarete were introduced at a post-opera supper party at the Sacher Hotel in Vienna where they shared their love of music. Arthur was a very competent violinist and played in the Vienna Medical School orchestra. In spite of the unsettled political situation, Vienna’s cultural life was still extraordinarily rich and the Schullers participated actively. They lived in a flat close to the university and the hospital and owned a house in Brunn and a weekend cottage by the Danube north of Vienna. They had a comfortable though not extravagant lifestyle. Indeed, the son of Arthur’s urologist cousin Hugo Schuller, who lived round the corner, reported that Arthur and Margarethe were somewhat parsimonious. Their two sons were born in 1908 and 1909. It may be that dedication to Arthur’s profession and his travel schedule had some impact on his relationship with Franz and Hans. It seems that they were closer to their mother’s family in Brunn than to the other Schullers in Vienna. They spent at least some of their teenage years living in Brunn with Margarete’s mother, to whom they were devoted, and both decided to join the family business rather than go to university, with fateful consequences.
Arthur’s 60th birthday. Grandmother and sons are highlighted. Arthur Schuller is 5th from right and his wife Margarete is 6th from right.
The unstable political situation in Vienna deteriorated further in the late 1930s and after the Anschluss in March 1938 life for Jews became very difficult. Although Arthur and Margarete had been baptised as Roman Catholics in 1908 the National Socialist decrees categorized them as Jews. As such Arthur was only allowed to treat other Jews and in April 1938 he was officially “sent on holiday” from the university along with more than half of the members of the Medical Faculty, a purge that effectively set the Vienna Medical School back 60 years. The Nazi rampage through Vienna in November 1938 persuaded the Schullers that it was time to leave. Dandy had invited them to go to the US but Arthur was concerned about growing anti-semitism in academic medical circles there and decided on Australia. It seems that he was encouraged by two Australians who had attended his courses in Vienna and were now significant figures in Australian medical circles. Both John O’Sullivan and Sydney Sunderland were in Oxford in 1939 and to Oxford was where the Schullers fled when their Australian visas and their German Reich passports and exit papers arrived in early 1939. Arthur had followed up on Cairns’ invitation and in April was welcomed and attached to the labs of Le Gros Clark in Anatomy and Barclay at the Nuffield Institute for Medical Research. While there Oxford Arthur wrote a paper on the sub-arachnoid cisterns and their demonstration using a positive contrast agent which was published in BJR in 1940, 13.(148):pps 127-29
The Symposium in Antwerp finished on 29 July, 1939 and in the first week of August the Schullers left Croydon airport on a KLM flight which took over a week and 30 stops to reach Darwin and then Brisbane and eventually on to Melbourne. Their arrival was noted in the press in the main Australian cities.
What the Australians had organised was a position at St Vincent’s Hospital in Melbourne run by the Sisters of Charity, which is where John O’Sullivan was based in the Radiology Department. Also at St Vincent’s was Frank Morgan the first specialist neurosurgeon in Australia. Schuller enjoyed spending time in both departments viewing and reporting on all head X-rays and attending Morgan’s ward rounds and operations. He was liked and respected by staff at all levels. Curiously, however, the Medical Board of Victoria did not recognise his University of Vienna qualifications and he was not formally permitted to practise in Victoria till 1946. He was lent rooms where he did see patients who were referred to him. He continued to write papers – his last was published in 1950 – and, although he declined to attend the second Symposium Neuroradiologicum in Rotterdam in 1949, he was elected Honorary President and the paper he submitted was given pride of place.
Dr Schuller and Dr Frank Morgan
In spite of his age Schuller’s attendance at St Vincent’s was constant, falling off only in his eighties. It was also stoical since on top of beginning to suffer from Parkinsons he had to bear the personal sorrow of family tragedy. Although they could have escaped, the Schullers’ two sons decided to stay in Brunn partly to care for their grandmother and partly to try to rescue the Stiassni family business. Both of them along with their grandmother and Hans’ wife and young daughter perished in Auschwitz in early 1943, though this news did not reach Australia till 1945. Arthur became increasingly depressed and even asked Morgan to perform a frontal lobotomy which Morgan refused to do. Arthur died in 1957 aged 83.
Margarete survived till 1971. She had taken to offering her services as a domestic help and, as such, worked for a number of Melbourne families. She cooked, ironed and looked after children. It is not clear why she did this. Since she left a substantial estate and her brother had continued to send monthly remittances from the USA financial need was probably not her main motivation. More likely she needed social company. She certainly embedded herself in some of the families for whom she worked. She was a devoted member of her local Catholic Church community.
Members of two of those families are featured in a 30 minute documentary film about the Schullers which is available for free viewing on YouTube at https://youtu.be/YhRLobn-Ubw
Also featured is Dr Keith Henderson who, as a young neurosurgeon at St Vincents, worked with and befriended Arthur. Henderson wrote a biographical memoir of the Schullers entitled Arthur Schuller Founder of Neuroradiology: a Life on Two Continents which Hybrid Publishers in Melbourne have just, in February 2021, published posthumously *. Henderson’s book contains substantially more detail about Schuller’s contributions to medical science than the film and it lists about half of the 300 papers he published.
Andrew Schuller was born in and educated at Oxford. He worked for over 30 years for Oxford University Press in New York and Oxford. Now retired, he spends much of the year in Australia and continues to be engaged in some publishing projects as well as family history. Andrew’s grandfather was a first cousin of Arthur Schuller, though it is not known if they ever met. By a strange series of coincidences, Andrew became involved in helping Keith Henderson in the writing of his memoir. It was at the suggestion of Austrian historians who have been recording the career and fate of Jewish medical practitioners in Vienna that Andrew embarked on making the film. He regrets that he did not know about Arthur much earlier when it would have been possible to talk to more people who knew him in Austria, Oxford and Australia.
Over the last 18 months, GenesisCare has treated more than 170 patients on the UK’s first ViewRay MRIdian MR-linac and adopted SMART planning as a new way of working. Here, Ben George explains why this latest hypofractionated technique has proven to be one of the success stories of the COVID-19 era.
Stereotactic ablative radiotherapy (SABR) is growing in importance in the curative cancer pathway. Increasingly, it offers patients the opportunity to enjoy relatively long periods of disease control where previously they would have been considered for palliative treatments. During COVID-19, the scales have tipped even further in favour of hypofractionated techniques because protocols have been revised to limit the risk of patient infection. More recently, attention has turned to stereotactic ablative MR-guided adaptive radiotherapy (SMART) – the most exciting development in radiotherapy for years, with the potential to treat previously inaccessible targets.
GenesisCare has been the first in the UK to adopt SMART, installing the first ViewRay MRIdian MR-linac just over a year ago. Since then, we have treated over 170 patients, some of which are the most challenging in the world from a radiotherapy perspective, such as pancreatic, central lung and now renal cell carcinomas. MRIdian sits within our SABR offering, which is run by a specialist team of oncologists, physicists, dosimetrists, and radiographers. Over an intensive 18 months, we have adopted a completely new way of working and overcome the challenges of a pandemic to treat patients not just from across the UK, but also from around the world.
SMART explained
The MRIdian MR-linac combines a 0.35 T split superconducting magnet with a 6 MV linear accelerator. This gives it unique advantages over conventional external beam radiotherapy linear accelerators, which rely on kV cone-beam CT (CBCT) imaging, and enables an entirely new approach to treatment.
First, using MRI instead of CBCT provides superior soft-tissue visualisation. This increased imaging capability allows the treatment to be adapted at each fraction based on the daily position of the target and nearby organs at risk (OARs). This is in marked contrast to external beam treatment with CBCT, where anatomy captured in the CBCT is simply rigidly matched against a planning CT. This rigid registration is then used to calculate the movements required to shift the patient into the correct position for treatment.
Second, the MRIdian takes images continuously throughout the treatment period to not only monitor the patient position, but also turn the treatment beam on and off. This is carried out as the patient’s anatomy moves through the breathing cycle.
This combination of enhanced visualisation and real-time imaging adds a layer of certainty in the delivery of treatment.
The MRIdian on-table adaptive planning system generates a new, optimised treatment plan for each fraction. This accounts for these day-to-day anatomical variations when the patient is in the treatment position.
Treatment delivery is then automatically gated so that the dose is only delivered when the target is in the optimal position. The machine is able to monitor every intrafraction motion caused by breathing or organ-filling.
As a result of these factors, we can design plans which deliver a higher dose, more precisely than with conventional SABR. There is no need for invasive fiducial marker insertion and any uncertainty is removed. Moreover, we can reduce planning target volumes, remove internal target volumes, and minimise the amount of tissue irradiated.
SMART has led to a paradigm shift in how some cancers are treated. In particular, it can benefit cancers in areas where there is significant inter- or intrafraction motion of either the target or OARs. Across the global community, MR-linac centres are now treating novel indications, such as renal, central lung and hepatobiliary tumours, and achieving clinical outcomes not previously thought possible. It is not simply a case of improving on an existing treatment – for some tumour types, SMART is facilitating new referral patterns for patients who may not typically be eligible for radiotherapy.
Pancreatic cancer – a new way of treating
Pancreatic cancer is one such example and of all the tumour sites we are now treating at GenesisCare, this is undoubtedly the one that is breaking most ground, offering new hope for both clinicians and patients.
For decades, surgical resection and adjuvant chemotherapy and radiotherapy have been the cornerstones of primary and secondary hepatobiliary tumours and pancreatic cancer treatment. However, options are limited for many patients. Less than 20% are resectable at diagnosis and not all patients are fit enough for an operation or effective chemotherapy regimens. There is, however, emerging evidence of a dose-response relationship, proving that escalated radiation doses are associated with improved local control as well as overall survival in borderline resectable (BRPC) or locally advanced pancreatic cancer (LAPC). Conventional radiotherapy delivers a comparatively homogenous radiation dose to the target volume. In contrast, SABR treatments combine advanced image guidance systems, accurate dose delivery and hypofractionated regimes. This is to facilitate a deliberate heterogeneous dose distribution across the target. This means the radiation tolerances of surrounding OARs are respected, while the tumour receives a higher, ablative radiation dose. A number of SABR studies have yielded good results in the treatment of large hepatobiliary tumours, with 1-year local control exceeding 90% and acceptable toxicity. Furthermore, delivering these hypofractionated ablative doses of radiation over a shorter treatment schedule has the potential to reduce the burden of treatment on patients.
However, with conventional SABR this therapeutic approach is often limited by concerns regarding organ motion and the possibility of developing small bowel radiation toxicity. As a result, many patients are only being treated with systemic agents. This is a prime example of where the elements of SMART on an MR-linac can facilitate an effective radiation dose escalation, while still respecting the radiation tolerance of normal tissues and surrounding OARs. In fact, using an MR-linac, it has been possible to successfully increase the prescribed dose in patients with primary pancreatic cancer. The previous standard dose was 33 Gy in five fractions, but SMART enables us to escalate the prescribed up to 40 Gy or even 50 Gy in five fractions. At the time of writing, 30 patients have been treated on the MR-linac for pancreatic tumours at GenesisCare.
Compassionate Access
The significance of MR-linac as an innovation in cancer treatment can’t be understated and, although at GenesisCare we are offering it in a private setting, we are committed to sharing the benefits of this technology with the wider medical community. Patients with localised pancreatic cancer have variable access to precision radiotherapy in the UK. The n-SARS-CoV-2 pandemic has further disadvantaged this patient group by reducing the availability and safety of surgery and chemotherapy. Considering this, since 2020 GenesisCare in association with GenesisCare Foundation, UK charity, Pancreatic Cancer Research Fund, ViewRay and University of Oxford have been treating NHS patients with localised pancreatic cancer with SMART at no cost. The programme, which is run through a partnership with the University of Oxford, is generating preliminary clinical and patient-reported outcome data on a UK cohort. This will inform the design of subsequent randomised clinical trials and help to embed SMART in UK oncology practice.
A new way of working
With any new technology, there comes a learning curve. MR-linac represents a significant change in working practices. It demands a style of inter-disciplinary working which challenges the norms.
In a standard radiotherapy workflow, a patient will receive a treatment planning CT one to two weeks before the start of treatment. During this time, several steps are carried out by a team of dosimetrists, physicists, doctors and radiographers to produce a treatment plan ready for the patient’s first fraction. These steps include contouring the treatment target and OARs and optimising the machine parameters to deliver the prescribed dose to the target while sparing critical structures. This is followed by reviewing the dose distribution, checking the planning process to ensure no errors have occurred and performing an independent dose calculation.
As part of the on-table adaptive workflow, the time taken for this process must be reduced from days to minutes. In order to achieve this, close inter-disciplinary working between the team is required. The need to undertake a number of complex tasks during each adaptive treatment also increases the time for each fraction to around one hour.
The MRIdian workflow involves a Clinical Oncologist on-site during treatment to oversee the daily adaption. To maintain a treatment schedule at GenesisCare, this has meant that clinicians had to be trained to contour all areas of anatomy, often working outside their main area of specialism. Equally challenging was the need to acquire skills in MRI interpretation, which for some specialities is not routinely used as a diagnostic modality. These were all skills that needed to be honed and validated before any patients could be treated on the MR-linac. In our case, we spent many hours learning with colleagues in MR-linac centres of excellence around the world. Twelve months later, we are experts in this field and have treated over 170 patients.
A body of evidence
There is a growing body of data as the global MR-linac community treats ever more and complex cases. We brought this international best practice to GenesisCare and have treated complex and challenging cases, including central lung, pancreas and reirradiation within our first year. We have many case studies available on our website genesiscare.com/mridian/case-studies. We already knew that the technology could deliver, but it was the confidence in our processes and the ability of our team to implement an adaptive workflow in a time-pressured environment, with a patient on the treatment table, which allowed us to embrace the opportunity that MR-linac presents in radiotherapy.
GenesisCare will install the second MR-linac in the UK in 2021. Through our MagNET programme, we are joining with NHS organisations to support education in the use of MR-guided radiotherapy. Enquiries to: James.Good@genesiscare.co.uk
Dr Ben George, Lead Physicist – MR Linac, GenesisCare
Ben is Lead Physicist – MR Linac at GenesisCare UK. He works as part of a multi-disciplinary team which has established a successful and world-leading SABR service delivering complex MR-guided adapted treatments. He has a PhD in Physics with a strong background in computer science, research and clinical computing. He has over ten years of experience as a Clinical Scientist specialising in radiotherapy in both the NHS and the private sector, and as a research scientist for the University of Oxford.
Angela Young explains how the process of making a podcast helped not only others with a diagnosed brain tumour but gave comfort and support to herself as she embarked on a course of radiotherapy.
A brain tumour diagnosis, like all major events, can set in place a chain of emotions, among them anger, fear and denial. It can also make you adjust your priorities in life. I went through all this in 2015 when I discovered I had a Grade 1 benign posterior fossa meningioma. A resection at Addenbrooke’s Hospital in Cambridge was very successful, leaving only a 3mm residuum.
I had been having regular follow up scans, and in 2019, it was thought the growth was significant enough to consider radiotherapy. After the initial shock, I realised that, if successful, it would prevent the cells from growing again and remove the need for annual scans with the associated “scanxiety”. My decision to go ahead now rather than wait for symptoms to appear was influenced by the consultant radiologist Dr Sarah Jefferies who said the benefit of doing so now was that I was “young and fit”, a nice thing to hear at the age of 59.
As a journalist and podcast maker, I am used to getting to grips with a variety of subjects quickly in order to explain them to others. It dawned on me that if I could tell the story of my own treatment, it would give me a sense of control over a process in which one can easily feel helpless. It might also provide information and some light relief to other people going through something similar and their families. The radiotherapy process would be the same for people undergoing treatment for a variety of conditions, not just brain tumours, and so creating a podcast on this topic could reach and potentially help a large audience.
I am very optimistic by nature and I like to see the funny side of things. I believe that if you look closely, you can find humour in most situations. Consequently, I decided the title of the podcast should be “A Sense of Tumour”. I started recording everything that happened, whether by phone call (I had got all the kit I needed for doing this when lockdown started) or recording my own commentary during appointments and tests and arranging interviews, either face to face (with masks on) or via an audio recording platform.
People find podcasts in a variety of ways. One of those is to have a well-known personality or influencer or support group post about them. It helps if you can interview a celebrity or two who will do this. When I asked Victoria Derbyshire (via a mutual friend) if she would talk to me about documenting her very public battle against breast cancer, I had no idea she would later be taking part in the TV programme “I’m A Celebrity, Get Me Out Of Here!”. Victoria appeared in Episode 1 and set the interview bar quite high. Luckily, the Brain Tumour Charity had come on board by this stage and offered to put me in touch with TV presenter Nicki Chapman, who had had a matching meningioma to mine removed last year. She readily agreed to be interviewed and candidly shared the highs and lows she experienced when going through treatment herself. For the final episode, I thought I would chance my luck and ask to speak to Tony Iommi, lead guitarist and song writer with Black Sabbath. He had had radiotherapy a few years ago and embraced some alternative therapies which I wanted to hear about. To my delight, he was more than willing to talk.
The series was meant to inform as well as entertain so I spoke to the medical professionals whom I was meeting and also those at the cutting edge of research into treatment. I interviewed the Chair of Cancer Research UK, Sir Leszek Borysiewicz, about funding for brain tumours. I also had conversations with the “Distinguished Scientist” from Elekta, one of the companies which makes the linear accelerator machine (not a bad job title!) and to many people from the team at Addenbrooke’s, including a medical physicist and a research radiographer. I learned a lot and I hoped that sharing these conversations would also help listeners to understand some of the more complicated parts of the treatment and process more easily.
Bringing the podcast’s listeners on my journey was supposed to feel personal too. I recorded as much as I could at every stage, including the baseline neurological assessment. This is an IQ-style test carried out before the start of a course of radiotherapy to the brain so that if there is any concern about future cognitive function, there is a baseline against which to compare it. One part of the test included listing as many words as possible beginning with the letter F; you can imagine what came to mind! When that episode was released, listeners I came across would shout out words beginning with F to me.
All the way through the treatment I was thinking how I would represent things aurally, such as the MRI machine. These make a variety of loud noises but would wreck any recording device in the vicinity. When I managed to open my eyes under the thermoplastic mask which holds the head in place on the linear accelerator, part of the machine going over me looked like a spaceship. Friends and family had each contributed a song for my radiotherapy playlist; that day the song was Mr Blue Sky and it had got to the instrumental part, which made me think of a science fiction movie. I was working out how to recreate the impression for the podcast. Thinking about this during the session took my mind off what was going on.
By the time you read this, I will have finished the treatment and will be waiting for a scan to see how successful it has been. I am, of course, hoping for the best. I would also like to think that the podcast series has been useful to patients and their families, to radiotherapists, to manufacturers and anyone else involved in this fascinating process. I also hope that it inspires anyone looking for a positive and creative way of dealing with a diagnosis of any kind to take control of what they can, focus on something meaningful and use their good days to bring strength to others. After all, positivity radiates.
Angela Young founded Cambridge Podcasts in 2018 to help clients showcase their expertise and establish themselves as the go-to person in their field. She is a former BBC radio journalist who has worked as a reporter, producer, news reader and news editor. She has taught law and journalism at the BBC and media handling at the prestigious Institute for Management Development in Lausanne. She studied law at Cambridge as a mature student and has lived in the city for 28 years. www.cambridgepodcasts.co.ukinfo@cambridgepodcasts.co.uk
What do tiny bees and dead salmon have to do with the history of MRI? This post by Dr David Higgins and Dr Matthew Clemence explores how the flexibility of MRI lends itself to important applications outside of medicine and examines how the use of functional MRI has more recently brought us much closer to real scientific observation of the brain.
MRI is a rapidly evolving imaging modality, and the history of MRI has always been intertwined with research. Its flexibility lends itself to fascinating applications outside of medicine; even bees, and fish.
In neurobiology, honeybees are a common model for analysing underlying neural mechanisms because of their simply structured nervous system. By investigating the bee brain’s anatomy, correlations between anatomy and function can be studied. See Haddad et al 2004 for MR images of tiny bee brains. One early project looked to see if there were any magnetic structures inside the bee – which MRI was uniquely sensitive to – that might help bees navigate. Bees have been studied by MRI surprising often, perhaps because their behaviour is extraordinary, emerging as it does from such apparently simple creatures. MRI has helped our understanding of this important crop animal (Tomanek et al, 1996).
Looking at the function of intact, living neuroanatomy has been a dream for students of the human mind for centuries. Phrenology (from Ancient Greek φρήν (phrēn) “mind”, and λόγος (logos) “knowledge”), which supposed that the lumps and bumps on the skull reflected personality traits, was developed in 1796 and remained influential up until the 1840s. While, in a marked understatement from Wikipedia, “the methodological rigor of phrenology was doubtful even for the standards of its time”, the underlying concept that that the brain is the organ of the mind – and that certain brain areas have localised, specific functions – is based in fact. Technology developments in electroencephalography, near-infrared spectroscopy and most recently functional MRI have brought us much closer to real scientific observation of the brain.
Which brings us to a dead salmon…
Functional MRI (fMRI) was a revolutionary technique used to identify highly localised changes in blood flow resulting from differential load on regions of the brain. John (Jack) Belliveau at Massachusetts General Hospital showed in a key Science paper that these changes could be measured with MRI (Belliveau et al, 1991) in conjunction with a Gadolinium contrast agent, but it was Seiji Ogawa who demonstrated a practical, non-invasive method with the University of Minnesota (Ogawa et al, 1990). For the first time, scientists had access to detailed 3D anatomical images of the brain in action, through a safe technique that could be repeatedly used on volunteers. Its ease of use, combined with wide availability, allowed the technique to be adopted rapidly in psychology and neuroscience, often in the hands of the non-MRI specialist. Some of the early studies exploring this new ability to “read minds” often drew overly broad conclusions from badly designed experiments. This almost relegated fMRI into a category of “modern phrenology”.
The dead salmon experiment showed how, with naive experimental design and data analysis, fMRI could give convincing results on a dead Atlantic salmon (Bennett et al, 2010) and was a salutary lesson to would be fMRI researchers to improve their methodology (Lyon, 2017).
Now, once again fMRI is being used to tease out our inner thoughts, whether to attempt to detect lying for legal purposes or read letters directly from the visual cortex. This could have a dramatic impact in patients with “locked in syndrome” through the development of brain computer interfaces (Sorger, 2010).
fMRI has also found an unusual application in neuromarketing: the application of neuroimaging methods to product marketing, to more effectively “match products with people”. Companies can incorporate use of fMRI in the design process of a product, as well as in assessing the effectiveness of an advertising campaign, even if the “product” is a political candidate. “Political marketing is aimed at selling an existing candidate but, with more foresight, can also be used to “design” a better candidate” (Ariely & Berns, 2010). Imaging our brains may reveal what we really think (or how we’re likely to vote), even if we can’t fully articulate our preferences yet.
If all this sounds hard to believe, perhaps a look at our brain scans could help you decide whether to believe us. “The relative reduction in prefrontal grey matter relative to white may also predispose to a general antisocial disinhibited tendency which, coupled with increased white matter, results in excessive lying.” (Yang et al, 2005).
Just check the study passes the dead salmon test!
To see how Philips can help you in neuroscience visit:
Ariely D & Berns G. Neuromarketing: the hope and hype of neuroimaging in business. Nat Rev Neurosci 2010;11:284–292. doi:10.1038/nrn2795
Belliveau JW et al. Functional mapping of the human visual cortex by magnetic resonance imaging. Science 1991;254:716-719. doi:10.1126/science.1948051
Bennett et al 2009. Neural correlates of interspecies perspective taking in the post-mortem Atlantic salmon: An argument for proper multiple comparisons correction. J Serendipitous Unexpected Results 2010;1:1–5. See https://www.nature.com/articles/nj7420-437a
Haddad D et al. NMR imaging of the honeybee brain. J Insect Sci 2004;4:7. doi:10.1093/jis/4.1.7
Lyon L. Dead salmon and voodoo correlations: should we be sceptical about functional MRI? Brain 2017;140;e53. doi:10.1093/brain/awx180
Ogawa S et al. Brain magnetic resonance imaging with contrast dependent on blood oxygenation. Proc Natl Acad Sci U S A. 1990;87:9868-9872. doi:10.1073/pnas.87.24.9868
Sorger et al. A real-time fMRI-based spelling device immediately enabling robust motor-independent communication. Curr Biol 2012;22:1333-8. doi:10.1016/j.cub.2012.05.022
Tomanek B et al. Magnetic resonance microscopy of internal structure of drone and queen honey bees, Journal of Apicultural Research, 1996;35:3-9. doi:10.1080/00218839.1996.11100907
Wikipedia contributors. “Phrenology.” Wikipedia, accessed 16 Oct. 2020. Yang Y et al. Prefrontal white matter in pathological liars. Br J Psychiatry 2005;187:320-325. doi:10.1192/bjp.187.4.320
Dr David Higgins and Dr Matthew Clemence are Senior Scientists at Philips, part of the UK&I MR Clinical Science team and the wider global Philips Clinical Science group. They provide: MR physics support; advanced teaching on the functions of the MR system; prototype pulse sequence deployment and monitoring; novel pulse sequence development advice; guidance for novel image reconstruction and analysis projects; advice for novel interfacing novel hardware.
Jeroen van Duffelen proposes a five-step programme for adoption of artificial intelligence in clinical practice.
Adoption of medical imaging AI is about getting your hospital or screening programme ready to implement the right solution for a clinical need. Running into speed bumps along the way is common for early adopters. How do you define the needs, budget, and outcomes? Which boxes should you check when selecting vendors? How do you manage internal stakeholders? The adoption curve is steep. Luckily, you don’t have to climb it alone.
Drawing from our experience deploying AI in clinical practice and lung cancer screening, I’ve designed a five-step guide to streamlined adoption. If you’re looking to adopt artificial intelligence but don’t know where to start, these actionable tips and advice will see you through. For the video breakdown of the steps, watch this presentation from ECR 2020.
1. Consider
Where do you start working with AI? First, look away from all the solutions out there, and focus on your organisation. Bring together all the stakeholders into a project team that includes the sponsor, if applicable, IT and legal representatives. Involving them from the beginning will expedite the process.
Start with defining the challenge you are looking to solve, or the specific clinical question that is relevant to your workflow. Some hospitals are looking to experiment with the technology, while others aim to solve a particular issue. Over the past years, I have seen the latter getting more out of AI, which is why my advice is to start from a clinical challenge.
When considering this challenge, make sure to already determine your expected outcomes. When is the adoption a success? Are you aiming to have an AI solution in use? Should it apply to a certain patient population, or yield specific results like time or cost savings?
Also, although it may seem early, this is also the stage to organise a budget dedicated to the AI solution. The size of this budget should relate to the cost or time savings a solution is expected to bring. Both the amount secured and its source will impact the next steps. For example, it will guide you to look for PhD researchers versus seeking a vendor that offers a mature solution.
2. Evaluate
The AI in healthcare space is widely populated; a Google search or a look at the list of vendors at the RSNA can confirm that. To weigh the existing options for your scope, do your (desk) research using this high-level checklist for each solution:
How was the AI solution validated?
It is important that the claim that the AI solution has validated covers the use case you identified in the previous step. Take the time to understand if the manufacturer has done studies confirming this claim.
How does it integrate into the workflow?
Try to get a feel of the amount of effort needed to add an AI system into your workflow. A good practice is to start with an AI solution that is easy to integrate with the current workflow and IT infrastructure. Workflow integration is of utmost importance for the radiologist; in this article, we explained why that is and how it works.
What regulations does the solution fulfill for use in clinical practice?
Commercialising medical devices requires a CE Mark in the EU and an FDA clearance in the US. Note that local regulations may apply to different countries. Again, pay attention to which claim is covered by the acquired certification.
3. Choose
By this stage, you should have narrowed your search down to a few vendors. This is the moment to go in-depth into the workflow and test if a specific solution is a good fit from both a clinical and a technical standpoint. A well-integrated AI system should not create hurdles for physicians, such as requiring them to leave their workstation to upload studies. It should further blend within the existing IT infrastructure.
There are two checks that are vital to make the right choice:
Validate the accuracy
Legitimate vendors would have done a study and can provide a clinical background for accuracy. To know if the solution is good at performing the defined task for your organisation, ask questions about the datasets used to develop and test the AI solution.
There are three datasets required to build an AI model: a training dataset, a validation dataset, and a test dataset.
The test dataset is the most relevant to look at because it is what the accuracy is based on. The performance on this dataset should be applicable to your hospital, with its specific protocols, type or number of scanners, and patients. To achieve this, the test set must cover the patient population your organisation serves (e.g. types of patients, comorbidities distribution, etc.). Thus, inquire about the specifics of the test set and the performance of the AI model on this dataset.
Secondly, you may want to know what the size of the training dataset is and how it was labelled. Both quantity and quality are important to train an accurate AI model. Labeling the data should be done by experienced radiologists, preferably with multiple readers per study.
Check the regulatory compliance
In Europe, medical device classification is divided up between risk Class I, Class IIa/b, or Class III. If looking for a solution for clinical practice, be wary of Class I medical devices. The new Medical Device Regulation, which will come into force in May 2021, will require many AI products currently classified as Class I devices to update their classification. For instance, software that supports diagnostic decisions should fall under Class II at a minimum. For more guidance on the new regulation, read our recent expert piece.
Apart from the regulatory approval, check if the vendor also has a quality management certification (e.g. ISO 13485). Reviewing the data processing policy and the cybersecurity measures in place will further help you understand if the AI company is going the extra mile in regard to safety.
A bonus tip for the choosing stage: do a reference check. Ask other organizations how they are working with the AI solution you have chosen. You may get the insights you need to make the final decision.
4. Approve
Approving the chosen solution internally requires the involvement of and coordination between IT and PACS administrators, procurement officers, physicians, often also privacy departments and legal officers. If you have a project team in place since the first step, you should be well on track.
To move forward and avoid delays, assign an internal AI champion responsible for driving the project. This may be an executive sponsor, a budget holder, or a department manager. One of my learnings from past deployments is that the risk of failure is high without a person fulfilling this role. What I have further learned as vendors is the importance of empowering the AI champion, by providing the necessary information and documentation in a timely manner.
Furthermore, make sure end users are trained to use the new medical device. If they don’t benefit from it, the impact of the AI solution will be limited. Additionally, setting up a feedback mechanism with the AI vendor from the get-go will help improve the AI product.
5. Deploy (& evaluate)
All the paperwork is signed – well done! To make the deployment work, create a clear project plan, including actions, timelines, and owners. Depending on the type of deployment – on-premise or cloud-based – different actions will be needed. As outcomes, set the deployment and acceptance dates, make agreements on the service levels, fixes, and upgrades, and discuss post-market surveillance.
The initial or trial phase of using the AI solution should show if it answers the problem you were trying to solve. It is a good moment to revisit step one and start evaluating the results to decide if you will continue using the solution.
A common question I get at this stage is: “Do I need to do a full clinical study?” The answer fully depends on the purpose of using the product. It is necessary for research, but not for other use cases. What matters is validating that the AI solution is adding value to your clinicians and their patients.
Make it better
AI adoption does not end with deployment. Service and maintenance are essential, and their quality often a differentiating factor between AI vendors. The implementation process usually acts as a good test for the AI companies fulfilling their promises and being prompt when handling requests.
Beyond these five steps, you and your organisation play a role in improving the chosen AI solution through valuable feedback and feature suggestions. The collaboration between humans and software allows us to achieve much more than humans would on their own. If done right, it can be transformative for patients.
Are you ready to start the AI journey? Get in touch!
Jeroen van Duffelen, COO & Co-Founder
Jeroen van Duffelen is COO and co-founder of Aidence. Jeroen’s entrepreneurial spirit led him to teaching himself software engineering and starting his own company commercialising an online education platform. He then tried his hand in the US startup ecosystem where he joined a rapidly scaling cloud company. Jeroen returned to Amsterdam where he ran a high-tech incubator for academic research institutes, it is here Jeroen first got his taste for applying AI to healthcare.
Dr Lizzie Barclay explores how artificial intelligence can influence lung cancer screening.
Radiology as the starting point
Imaging plays a fundamental role in lung cancer screening programmes. So, when it comes to improving technology to support the programmes, the radiology department is a good place to start.
The goal of screening is to pick up early cancers which can be treated and potentially cured, therefore improving patient outcomes (as outlined in the NHSE long term plan). Low dose CT has been shown to provide sufficient image quality for detection of early disease, whilst minimising radiation dose in asymptomatic individuals. Thoracic radiology expertise is required to determine which lung nodules may be malignant and therefore require invasive investigation, and which are likely benign and can be monitored with intermittent imaging. Appropriate follow-up recommendation helps avoid unnecessary invasive procedures, such as biopsies, and minimise patient anxiety, which are important measures of the efficacy of lung cancer screening programmes.
End to end lung cancer screening involves input from many healthcare professionals, and intelligent computer systems across specialities would benefit multidisciplinary teamwork. Thus, beyond image analysis, there are many opportunities for technology to add further support for effective and sustainable screening programmes. For instance, it could aid in the optimisation of image acquisition, access to imaging reports and relevant clinical details, tracking patient follow up, or in communication between patients and GPs.
Where AI-based image analysis makes a difference
Reading and reporting CT scans is time-consuming, and within a workforce which is already under strain, introducing a new CT-screening programme seems like a tall order. AI-driven solutions can support radiologists and contribute to successful lung cancer screening by bringing improvements in three areas:
Performance
Computer intelligence can increase the performance and productivity of CT reporting, freeing up time for radiologists to spend on clinical decision making and complex cases. Specifically, AI software is well-suited for precise:
Detection of elusive lung nodules, and differentiation of subtle changes
Automatic volume measurements, to help determine the appropriate frequency of monitoring (e.g. stable vs growing nodule, according to the BTS guidelines).
What further distinguishes computers from humans is the absolute consistency in their high performance, without being impacted by common external stressors to which a radiologist would be exposed (e.g. time-pressure, workload and interruptions).
(E)quality
Having a ‘second pair of eyes’ looking at the scan can increase the confidence of the radiologist in their own assessment. Additionally, making the AI-driven, accurate measurements available regardless of the level of expertise of the reporting radiologist could not only benefit quality assurance, but also equality within the radiology department. The use of AI would reduce the need for all scans to be reported by the most experienced thoracic radiologists with interest in early lung cancer detection, and instead facilitate spreading the workload across the workforce.
Another use case concerns quality assurance when outsourcing to teleradiology companies. AI-based image analysis can improve consistency of reporting, drive the recommended terminology use, and, essential for lung cancer screening, ensure access to relevant prior imaging for comparison and change assessment over time.
Efficiency (via integration)
An intelligent computer system should not slow down reporting turnaround times, but improve efficiency, as well as quality, to ultimately minimize time to diagnosis (for example, the NHSE long term plan introduces a 28-days standard from referral to diagnosis or rule out).
Older CAD technology was often described as ‘clunky’ – requiring images to be uploaded to separate systems for analysis. Additional manual steps between image acquisition and the radiology report make the process time consuming, and often require radiology support staff to manage the workflow. It is important to consider allocative and technical efficiency which play important roles in the evaluation of screening programmes, and their impact on healthcare systems.
An AI-driven image analysis software which is fully-integrated in the radiologist’s pre-existing workflow can provide automatic results, without needing additional departmental resources. An additional benefit of fully-integrated AI solutions is that their use is not restricted by time or place, therefore supporting flexible and remote working. In the context of the COVID-19 pandemic, it’s been encouraging to see the increase in remote reporting, whilst maintaining a functioning department, in many hospital trusts. Going forward, it will be interesting to see whether radiologists will have the option to continue to work remotely where possible.
Valuing input from healthcare professionals
New lung cancer screening programmes will be monitored regularly to evaluate their effectiveness and determine areas for review. Commitment from all parties to work together will facilitate optimisation of the pathway to achieve better patient outcomes and positive impacts on healthcare systems.
In our experience, close collaboration between medtech and healthcare professionals is important for learning lessons along the way. Understanding radiologists’ needs helps tech teams develop a clinically valuable tool.
For example, Aidence’s interactive lung nodule reporting tool, Veye Reporting, was designed based on the needs of radiologists involved in reporting lung screening scans. From our conversations with them, we understood that following the detailed and complex reporting protocols in lung cancer screening programmes make for labour-intensive, repetitive tasks.
To help them produce reports that follow the standardised NHSE proforma and facilitate audit for quality assurance, we added Veye Reporting as a feature to Veye Chest, focusing on making it easy-to-use and efficient. With this tool, the radiologists further have control over which nodules to include in the report, different sharing options, and the choice to add incidental findings.
What’s next?
Cancer services have been impacted by the COVID-19 health emergency. In the UK, screening has been paused and planning to (re-) start at the end of 2020 or beginning of 2021. Talks of introducing screening are ongoing in various European countries, as are concerns of catching up with the backlog of screening scans.
The British Society of Thoracic Imaging and the Royal College of Radiologists released these considerations for optimum lung cancer screening roll-out over the next five years. Their statement below is a reminder of why it is worth overcoming challenges and leveraging technology to make screening programmes a success:
Dr Lizzie Barclay, Medical Director
Dr Lizzie Barclay’s areas of interest are thoracic radiology and medicine, innovation, and improving patient outcomes and healthcare professionals’ wellbeing.
Lizzie is originally from Manchester, UK. After graduating from the University of Leeds Medical School (MBChB), and Barts and the London School of Medicine (BSc sports & exercise medicine), Lizzie spent four years working as a doctor in Manchester and Liverpool NHS Trusts, including two years in Clinical Radiology. She has presented her work on lung cancer imaging at national/international conferences, and recently contributed to Lung Cancer Europe’s “Early Diagnosis and Screening” event at the EU Parliament in Brussels.
100 years ago the UK was facing a fast-moving outbreak of epidemic influenza pneumonia, known as the “Spanish Flu”.
Radiology played an important part in diagnosis, although the crisis was without the scientific knowledge, strategic management and communications we have today. Here, Dr Adrian Thomas explores the six patterns of infection in this unpredictable and powerful disease.
Radiology is playing a central role in the diagnosis of COVID-19 today, and 100 years ago was also playing an important role in the diagnosis and characterisation of the outbreak of epidemic influenza pneumonia of 1918–1920. A combination of fluoroscopy and radiography was then used, with the occasional utilisation of stereoscopy. The greatest pointer to a diagnosis of epidemic influenza pneumonia in a given patient was the presence of the epidemic, although there were some specific features to indicate the diagnosis. The etiological cause of influenza was not known at the time, being first discovered in pigs by Richard Shope in 1931.
The epidemic of 1918 far exceeded previous ones in its intensity. It had a high mortality in young adults with the very young and very old being comparatively immune. The associated pneumonia was particularly virulent. In the case of the troopship The Olympic (sister ship of The Titanic) there were 5,951 soldiers on board. Initially there were 571 cases of acute respiratory disease, but within 3 weeks there were 1,668 cases. Of these, 32% had pneumonia, of which 59% died. In any locality the duration of the epidemic was from between 6–8 weeks, and approximately 40% of the population was affected (Osler, 1930).
Six patterns of infection were identified, with correlation of clinical, radiological and post-mortem findings (Sante, 1930., Shanks, et al. 1938). Dr Leroy Sante, the pioneer radiologist from St Louis, described epidemic influenza pneumonia as “the most lawless of the chest infections.” Abscess formation was seen frequently, and was commonly of the small and multiple type. Radiological changes were seen developing day by day, and clinical resolution needed at least six–eight weeks since there had commonly been lung destruction and healing by fibrosis needed to occur.
The patterns were:
Type 1: Peribronchial invasion with infiltrates that enlarge and become confluent forming small areas of consolidation (figures 1 & 2, below). This was not confined to one lobe, but could appear in all lobes as a true bronchopneumonia. This was similar in appearance to ordinary bronchopneumonia.
Figure 1
Figure 2
Type 2: Peribronchial invasion with infiltrates that enlarge and become confluent to form solidification of an entire lobe (figure 3, below). The changes remained confined to a single lobe. It was viewed as a true bronchopneumonia but with a lobar distribution (“pseudolobar pneumonia”). Different lobes may be invaded one after another. The pseudolobar pattern was the commonest type, and could resolve without further spread. The presence of previous isolated infiltrates would distinguish this type from common lobar pneumonia. There was a tendency to break down with extensive cavitation.
Figure 3
Type 3: This starts as blotchy infiltrates that coalesced to form a general haziness over a part of a lung, suggesting a haematogenous origin (figures 4 and 5, below). At post-mortem this was found to be an atypical lobular pneumonia, a “diffuse pneumonitis”, that was so commonly seen during the influenza outbreak. It resembled the streptococcal (septic) pneumonia that was often seen in association with septicaemia when there was no epidemic. The spread was rapid, and the prognosis was poor. Death commonly occurred within the week.
Figure 4
Figure 5
Type 4: A type starting in the hilum and spreading rapidly into the periphery, the so-called “critical pneumonia” (figure 6, below). This was attended with a high mortality. Post-mortem showed a purulent and haemorrhagic infiltration around the larger bronchi. There was often marked cyanosis.
Figure 6
Type 5: This started in the dependent part of the lungs, with continuous upwards spread (figures 7a and b, below). This was an atypical lobular pneumonia, there was no associated pleural fluid, and it was usually fatal. Initial infection in the costo-phrenic angle spread within 24 hours to involve the lower lung, and death occurred within 48 hours. Clinical features included extreme prostration, high temperature, and delirium. This pattern with rapidly advancing consolidation was seldom seen in other conditions.
Figure 7a
Figure 7b
Type 6. A true lobar pneumonia was only seen rarely.
The prognosis of epidemic influenza pneumonia was difficult to determine. So, as an example, a patient who was resolving would suddenly have changes extend into the other lung and then die. Another patient with successive involvement of all lobes could recover completely. A patient with only minor lung involvement might die, and another with extensive consolidation would recover completely.
Radiologists continue to be in the front line in the treatment of infectious diseases, and although our modalities are now more advanced than a century ago, their contributions remain essential. It is also noteworthy that the simple CXR also remains central.
Figures:
1. Type 1, Influenza bronchopneumonia. Image seen as a positive.
2. Type 1, Influenza bronchopneumonia. Peribronchial clusters of infiltration, with no relation to lobar architecture. Viewed as from behind.
3. Type 2, or pseudo-lobular.
4. Type 3, resembling streptococcal (septic) pneumonia. Image seen as a positive.
5. Type 3, resembling streptococcal (septic) pneumonia. Blotchy ill-defined infiltrates which coalesce to form a general haziness. Viewed as from behind.
6. Type 4, the so-called “critical pneumonia.”
7a. Type 5. This started in the dependent part of the lungs, and this early film shows consolidation in the costophrenic angle (black arrow).
7b. Type 5. A film taken 12 hours after 7a. The lower right lung is consolidated, and the patient died 12 hours later. Post mortem showed a solid lung with no effusion. Readings:
Osler, William. (1930) The Principles and Practice of Medicine. 11th Edition, Thomas McCrae (Ed.). London: D Appleton.
Sante, Leroy. (1930) The Chest, Roentgenologically Considered. New York: Paul B Hoeber.
Shanks, S Cochrane., Kerley, Peter., Twining, Edward W. (Eds). (1938) A Textbook of X-ray Diagnosis by British Authors. London: H. K. Lewis.
Dr Adrian Thomas FRCP FRCR FBIR, BIR Honorary Historian
About Dr Adrian Thomas
Dr Adrian Thomas is a semi-retired radiologist and a visiting professor at Canterbury Christ Church University. He has been President of the Radiology Section of the Royal Society of Medicine, and of the British Society for the History of Medicine. He is the Honorary Historian to the British Institute of Radiology. He has had a long-term interest in role development in radiography, and teaches postgraduate radiographers.
Adrian has written extensively on the history of radiology writing many papers, books and articles. He has, with a colleague, written a biography of the first female radiologist and female hospital physicist: Adrian Thomas and Francis Duck: Edith and Florence Stoney, Sisters in Radiology (Springer Biographies) Springer; 1st ed. 2019 edition (1 July 2019).
Do you ever wonder how you got where you are? Are you sure you see yourself as others do?
Dr Elizabeth Loney, Consultant Radiologist and Associate Medical Director, reflects on imposter syndrome and offers tips on how to manage it.
How many times have you sat in a meeting and looked around the room thinking, “what on earth am I doing here? Everyone else knows way more about this than I do, and they know it!”
The first senior management meeting that I attended started with reviewing the minutes of the last. As I read through the document, I realised I had no idea what much of it said—death by TLAs (three letter acronyms!). I nudged the person next to me and said, “what does … stand for?” They shrugged their shoulders and whispered to the person on their other side “what does … mean?” It took five people down the line before someone knew what it was! I found that reassuring, but also slightly scary. The fact that other people were in the same boat made me feel less like an idiot, but at the same time, how could such a senior group not understand the jargon and why had they said nothing? So… lesson one: be curious and not afraid to ask questions. You’re probably just asking what most people are thinking anyway!
About six months ago I started the Nye Bevan Programme with the NHS Leadership Academy. If I pass, I will allegedly have proven myself ready for an NHS executive leadership role. There are around 48 others in my cohort, all senior leaders in different areas of the NHS. What the heck am I doing there?! I’m just a doctor, not a leader. I might sort things out for people as Clinical or Divisional Director but I’ve never felt more like a “public servant” than when in a “leadership role”. I had serious Imposter Syndrome. The first residential was entitled “Knowing Yourself and Others” and was all about the impact you have on others as a leader and why you act as you do—unconscious bias and all. It was a traumatic experience for me. I did so much “reflecting” I felt like a mirror! I couldn’t do it—just give me a few scans to report! I’m not a leader—get me out of here. However, I got chatting to others that week and realised that pretty much everyone else in the room felt the same. Most people suffer with this issue at some time—and if you don’t, why not? A little humility is a wonderful thing.
Are you affected by low self-confidence? At times like this, seeking peer feedback can be helpful. As part of the course I had to send out a questionnaire asking others I had led on a work programme for anonymous feedback. That was scary! I asked questions including “what do I do well?” and “what could I do better?” I half expected to be slated but, to my surprise, the feedback was really positive. My view of myself was distorted. I may not see myself as a leader but apparently others do! So… lesson two: when you feel like an imposter remember that many others in the room feel the same way. There must be a reason why you are there. What do others see in you, that you do not? What is your role in the group? ‘If not you… who?’
So ends my first blog as Chair of the BIR Leadership and Management SIG… another position I find myself in wondering how I got here! What do I know about leadership? I’m not an expert. However, I do have a passion for self-improvement and a curious nature. Why not join me on my journey to “managerial enlightenment”? We have such a lot to learn from one another.
I hope to meet you in person at the BIR Annual Congress where we will gain inspiration from excellent speakers covering topics on “practical” and “personal” management, including an interactive session by Philips based on their “Insights” programme—expect to be up on your feet! We are also holding our first annual event on leadership, “Leadership 2020” on 31 January 2020. Come along and join us for more opportunities to learn, network and ask questions.
See you there!
Dr Elizabeth Loney,
Chair of the BIR Leadership and Management Special Interest Group
Dr Elizabeth Loney is Chair of the BIR Leadership and Management Special Interest Group (SIG). She is a Consultant Radiologist and Associate Medical Director and Consultant Radiologist at Calderdale and Huddersfield NHS Foundation Trust.
Dr Deepsha Agrawal reflects on how a taster week at her local hospital was the first step on her journey to qualifying as a radiologist.
Having read several narratives of Röntgen’s glowing cardboard screen and the mysterious Crooke’s tube, I have always found myself fascinated by radiology. I often wondered what radiologists do in their secretly tucked away dark rooms and how those digital blueprints and monochrome scans make sense. The evolution of radiology from giant X-ray tubes to present day dynamic scans and angio seals, prompted me to consider a career in radiology. And so valuable was my taster week experience that my interest has now transformed into a drive to become a radiologist.
I am an international medical graduate doing my Foundation Year 2 Clinical Fellowship. Although I had done a two week elective in radiology during my internship (the Indian equivalent of FY1), I was keen on doing a taster week before entering specialty training in the UK.
How I arranged it:
A taster week can be a great opportunity to give a useful insight into a specialty and connect to trainees and consultants who are currently working in the specialty. I arranged my taster week by emailing a radiology consultant in my hospital who kindly accepted and set things up for me promptly.
After a quick discussion with the radiology consultant, I emailed my rota manager who was very generous to grant me study leave for a week.
My experience:
My week was spread between plain film, ultrasound, CT, MRI and some interventional radiology sessions. While the plain film sessions were useful to carry into my regular job, the IR experience in the theatre was quite thrilling. Interventional radiologists are clinicians with those magic wands (catheters) who practice some seemingly futuristic medicine. It was an absolutely inspiring experience for me.
Spending a week in radiology gave me a lot of clarity on my doubts and misconceptions about the specialty.
Artificial intelligence (AI) won’t replace radiologists: Every time I had expressed my interest in radiology, I was told that it will soon be replaced by AI and radiologists will be left with no jobs. My experience tells me that AI will only alter the job of a radiologist and not replace it. Radiologists do more than reading and interpreting images. They recreate the patient’s clinical story when they look at a scan. AI can recognize but never interpret an image.
Radiology is a core clinical specialty: I was under the impression that radiology is mainly technical and has only a slight clinical edge to it. During one of my initial sessions I mentioned the same to a radiology consultant and amusingly but legitimately he got quite upset and told me there’s a reason it’s called “Clinical Radiology”. A week into radiology, I realised that there is in-depth clinical processing in radiology with every scan.
Radiologists touch the lives of their patients every day: It might be true that radiologists see fewer patients than an average clinician but with every scan interpretation a radiologist is affecting the life of a patient. They add value by not only interpreting the scans but also consulting with other physicians on diagnosis and treatment, treating diseases with intervention and relating findings clinically and from lab tests.
More recognition within the healthcare system: I was fortunate to attend a surgical and respiratory Multi-disciplinary Team Meeting (MDT) during the week. These meetings gave me insight into the role of a present day radiologist. The traditional view of the radiologist as a physician who sits in the dark room defining technical parameters of imaging procedures and interpreting diagnostic images is now outdated. Radiologists have now come to the forefront with multi-disciplinary meetings where they are valued and recognized for their opinion in deciding the course of treatment for patients.
Radiologists are happy people: Having rotated through various departments during my internship and experiencing a few departments in the NHS, I found a striking difference in how radiologists see their work. They work as a team, care for each other and are very encouraging. Don’t be surprised if your fellow consultant is making you a cup of coffee! Also, the trainees fairly support medical students and junior doctors in walking the path to enter specialty training. Overall, I felt that the happiness index of radiologists was higher than other specialists and they truly enjoy their work.
Although I entered as a slightly confused junior doctor, I have come out more aware and orientated to work towards a career in radiology with audits, academic projects and day-to-day learning ideas. In summary, I thoroughly enjoyed my taster week and am pleased with my experience. For a radiologist, no two days are the same. There is immense learning and fun in radiology. I am already dreaming of holding the needles and being on the dictaphone. I highly recommend a taster week to all junior doctors considering a career in this specialty.
I would like to add a special note of thanks to Dr. Amit Patel, Consultant Radiologist, Queen Elizabeth University Hospitals, Glasgow, who kindly accepted me as a taster week student and scheduled my sessions.
– Deepsha Agrawal, FY2 Clinical Fellow, Neurosurgery, Queen Elizabeth University Hospitals, Glasgow.
About Deepsha
I am an FY2 Clinical Fellow in Queen Elizabeth University Hospital in Glasgow. After graduating from India in 2018, I moved to the UK for further training with a keen interest in Radiology. My journey has been great so far and I look forward to bringing innovations to medicine as a radiologist.
Physicist Andy Moloney and Clinical Oncologist David Morgan reflect on how radiotherapy developed since their early careers
We first met in the autumn of 1981, when the NHS was, at 33 years from its inception, but a youngster. Andy had recently joined the Radiotherapy Physics staff at Nottingham General Hospital after graduating in Physics from the University of Nottingham, and David was returning to the clinical Department of Radiotherapy and Oncology after a year’s Fellowship at the Institut Gustave-Roussy in France. A firm friendship rapidly developed, one that continues to this day.
On reflection, joining the radiotherapy fraternity at that time was a leap of faith. The perceived wisdom amongst many of our scientific and clinical colleagues at the time was that this treatment technique was outdated and overshadowed by radical surgical procedures, new chemotherapy agents and biological modifiers poised to reduce radiotherapy to the history books.
This was a time when, in this Cinderella of specialties, physics planning was achieved by the superposition of two dimensional radiation plots (isodoses) ,using tracing paper and pencils, to produce summated maps of the distribution. The crude patient outlines were derived from laborious isocentric distance measurements augmented by the essential “flexicurve”. The whole planning process was slow and labour intensive fraught with errors and ridiculed by colleagues in the perceived prestigious scientific and clinical disciplines. The principal platform for external beam radiotherapy delivery, the Linear Accelerator (LinAc), had also reached something of a plateau of development, albeit with improved reliability, but few fundamental changes. Caesium tubes were transported from the “radium safe”, locked in an underground vault, to the operating theatre in a lead-lined trolley, where they were only loaded into “central tubes” and “ovoids” after the examination under anaesthetic (which was performed with the patient in the knee-chest position); they were then manually placed into the patient, who went to be nursed on an open ward, albeit behind strategically placed lead barriers.
For no sites outside the cranium was Computer Tomography (CT) scanning available. Magnetic Resonance Imaging (MRI) was still a vision seen only by a small number of enthusiasts.
All these limitations were met by a developing team of scientific and clinical enthusiasts believing in the future of radiotherapy if only technology could deliver solutions to address an improving understanding of the differing cancers and their radiobiology.
In the latter half of the eighties these solutions began to crystallise. Computers were being introduced across the NHS and their impact was not lost in radiotherapy. Pads of tracing paper were replaced with the first generation of planning computers. The simple “Bentley-Milan” algorithms could account for patient outlines accurately and speedily and optimising different beam configurations became practical. Consideration of Organs at Risk, as defined by the various International Commission on Radiation Units (ICRU) publications, became increasingly relevant. Recognition of the importance of delineating the target volumes and protecting normal tissue required improved imaging and this was provided by the new generation of CT scanners. In the nineties these were shared facilities with diagnostic radiology departments. However, the improvements provided by this imaging, enabling accurate 3-dimensional mapping of the disease with adjacent normal tissues and organs at risk, dictated their inclusion into every radiotherapy department soon after the millennium. The added bonus of using the grey scale pixel information, or Hounsfield numbers, to calculate accurate radiation transport distributions soon followed when the mathematical and computer technology caught up with the task. The value of MR and Positron Emission Tomography (PET) imaging was also recognised in the diagnosis, staging and planning of radiotherapy and the new century saw all of these new technologies embedded within the department.
Mould room technology was also improving with “instant” thermoplastic immobilisation shells replacing the uncomfortable plaster and vacuum forming methods. Custom shielding with low melting high density alloys was becoming routine and it was not long before these techniques were married with the emerging CT planning to provide “conformal” treatments.
LinAc technology also received added impetus. Computers were firstly coupled as a front end to conventional LinAcs as a safety interface to reduce the potential for “pilot error”. Their values were soon recognised by the manufacturers and were increasingly integrated into the machine, monitoring performance digitally and driving the new developments of Multi Leaf Collimators (MLC) and On Board Imaging (OBI).
The dominos for the radiotherapy renaissance were stacked up, but it needed the radiographers, clinicians and scientists to decide on the direction of travel. Computer power coupled with advanced electro-mechanical design had transformed MLC efficiency and resolution. Conventional conformal planning was now progressively superseded by sophisticated planning algorithms using merged CT and MR images. Intensity Modulated RadioTherapy (IMRT) had arrived in its evolving guises of multiple fixed field, dynamic arc therapy (RapidArc) or Tomotherapy. Whichever technique, they all offered the radiotherapy “Holy Grail” of providing three dimensional homogeneous dose distributions conformed to the Planning Target Volume (PTV) whilst achieving the required dose constraints for organs at risk and normal tissue preservation.
The tools had arrived, but an infrastructure to introduce these “toys” safely into a complex clinical background had also developed alongside. Quality standards (ISO9000), Clinical Trials, Multi Disciplinary Teams and Peer Review were governance mandates for all oncology departments and radiotherapy was leading the way. In forty years, radiotherapy had lost the “Cinderella” image and had been invited back to the clinical ball. Noticeably, breast and prostate adenocarcinoma constituted half of the radical workload.
The question remains of how and why did this transformation occur? Obviously the developing computer power and technology were the pre-requisites for many of the developments, but a key catalyst was the foresight of all of the radiotherapy family from which enduring friendships have been forged. The working lives of the clinicians and physicists involved in radiotherapy planning have probably changed more dramatically than those of any other medical and paramedical groups over the last 35 years.
We may have retired, but we still cogitate about the future direction and science behind this developing and essential cancer treatment and look forward to our younger colleagues enjoying their careers as much as we enjoyed ours.
About David Morgan
Dr David A L Morgan began training in Radiotherapy & Oncology as a Registrar in 1977, and in 1982 was appointed a Consultant in the specialty in Nottingham, continuing to work there until his retirement in 2011. He joined the BIR in 1980 and at times served as Chair of its Oncology Committee and a Member of Council. He was elected Fellow of the BIR in 2007. He is author or co-author of over 100 peer-reviewed papers on various aspects of Oncology and Radiobiology.
About Andrew Moloney
Andy Moloney completed his degree in Physics at Nottingham University in 1980 before joining the Medical Physics department at the Queens Medical Centre in the same city. After one year’s basic training in evoked potentials and nuclear medicine, he moved to the General Hospital in Nottingham to pursue a career in Radiotherapy Physics and achieved qualification in 1985. Subsequently, Andy moved to the new radiotherapy department at the City Hospital, Nottingham, where he progressed up the career ladder until his promotion as the new head of Radiotherapy Physics at the North Staffordshire Royal Infirmary in Stoke-on-Trent. Over the next twenty years Andy has acted as Clinical Director for the oncology department and served on the Radiation Physics and Oncology Committees at the BIR and was appointed a Fellow in 2007. He has been the author and co-author of multiple peer reviewed articles over the years prior to his retirement in 2017.
What does a jazz band, a ghost train and a figure in dark goggles have in common? They are all part of the NHS 70 memories of Professor Ralph McCready.
As a houseman I had the privilege of working for Professor Frank Pantridge, inventor of the defibrillator. I was fascinated by his catheter lab with the combination of physiology and radiology. So I decided to become a radiologist but was advised to go to England (from Northern Ireland) and obtain an impressive degree so that I could return if I wished. So I went to Guy’s Hospital, London to study for an MSc in Radiation Physics and Biology and the Diploma in Medical Radiodiagnosis (DMRD), paying my own fees.
Guy’s Radiology Department was interesting. The radiology chief was Dr Tom Hills who smoked cigars, had a tiny lead apron over the appropriate parts and had made an automatic wet X-ray film processing system.
It was obvious I would never get a radiology job at Guy’s coming from Belfast, speaking strangely, and not having the MRCP (Membership of the Royal College Physicians examination) so I applied for a Senior House Officer (SHO) position at the Hammersmith Hospital London where everybody was equal.
At the Hammersmith I was told by the other applicants that I would not get the job as I had come from Belfast. However I was determined to leave the interview with my head held high. I was first in to the SHO interview and was amazed to see a long row of people on the other side of the table headed by Professor Robert Steiner. He opened the questioning by asking why I was a member of the Musician’s Union. I explained that all my colleagues in the White Eagles Jazz Band had failed their exams, left the University and turned professional. To continue to play with them I had to join the Union. Then I was asked what else I had done, so rising to the occasion I told them I had been the ghost in a ghost train in an Amusement Park. I was bored so I connected the light over the skeleton to be permanently on. The little children came out saying that there was a ghost reading the Daily Telegraph beside the skeleton. Of course nobody believed them and the people outside poured in to see what was going on.
I emerged from the interview after forty minutes to tell the other candidates how awful the interview had been. I was appointed to the position! Professor Steiner used me to do all the odd jobs in the X-ray department for the next two years. As the junior doctor I worked in the dark with the oldest Watson X-ray set. Every time I took an erect X-ray the large steel edged cassette containing the film would slide across and usually fall out of the carriage landing on the floor with a loud crash frightening everybody in the darkened room.
It was a time of great innovation at the Hammersmith: the first renal transplant was carried out; micturating cystograms were started. After initial problems with old ladies standing up in the dark being unable to ‘pee’ when the urine hit the steel bucket with a tinkle, the problem was solved by lining the bucket with sound deadening polythene. Friday was ladies’ day when I was the only radiologist who performed Hysterosalpingography. It was done in a small room with a boiling water sterilizer in the corner. When I came out to view the films the steam poured out of the door and I would appear in a cloud of steam as a fearsome figure wearing large dark goggles and a long lead apron to the consternation of the waiting mixture of NHS and private practice ladies.
I graduated in Medicine from Queen’s University Belfast and then worked as a Houseman in the Royal Victoria Hospital. When I came to England I studied for the MSc in Radiation Physics and Biology and the Diploma in Radiodiagnosis at Guy’s Hospital London. After working as an SHO in Radiology at the Hammersmith Hospital I was appointed to a research position at the Institute of Cancer Research in Sutton, Surrey. With the development of a Nuclear Medicine Department at the Royal Marsden Hospital I became the consultant in charge for over 40 years. In 1987 I was awarded a DSc by Queen’s University Belfast, the British Institute of Radiology Barclay Prize in 1973, an Hon. FRCR in 1975, an Honorary Fellowship of the Faculty of Radiologists Royal College of Surgeons, Ireland in 1992 and made an Honorary Member of the Japanese Radiological Society also in 1992. I was appointed to a personal chair in Radiological Sciences in the Institute of Cancer Research in 1990.
As a founder member of the British Nuclear Medicine Society I have recently co-edited a book celebrating the 50th Anniversary of the Society and the development of radionuclide studies in the UK.https://link.springer.com/book/10.1007/978-3-319-28624-2
Kim Mason, an Audit and Research Radiographer for Mid Yorkshire Teaching Hospitals Trust, talks about their role as well as the value of radiographer engagement in research activities and how to get involved.
In December, 1895, Wilhelm Röntgen would x-ray the hand of Anna Bertha Ludwig, his wife, using a photographic plate. The new discovery lit a fire in the scientific community, and was so sensational that in the following year over 1,000 articles would be published on the topic of X-rays. Over the next 130 years, medical imaging has undergone many varied evolutions to become a cornerstone of modern-day medicine. All beginning with that first piece of research.
Radiography has exploded into a variety of modalities and specialisms from CT to Ultrasound to MRI; all driven by research and development. That is where I come in.
Hi, I’m Kim and I am an alternative-styled, funky-haired, septum-pierced, disabled Audit and Research Radiographer. That is to say, I’m fairly easy to pick out of a line up. I’m also passionate about education, research, and (of course) radiography. This, I’ve been told, is also very easy to pick up on.
I graduated with my radiography degree in 2018 and since then I’ve worked in a wide variety of departments, from plain film to nuclear medicine. Since I found something to love in every modality it never really mattered which one I was in. Prior to my current position, I’ve spent time as a Radiation Protection Supervisor, and well as a trainer for graduate and post graduate radiographers. Now I’m in Audit and Research, which is far different to anything I’ve done before.
So, what is an Audit and Research Radiographer?
Kim sat in their wheelchair at the UKIO 2023 conference
My position is entirely based in research so I do not currently undertake any non-research imaging. However, I’m not entirely non-clinical. I get trained to undertake research scans on new equipment as required for me to carry out the necessary imaging for research trials. I also provide support to all trials requiring access to our radiography department, regardless of the imaging modality.
My job requires that I read a lot of trial protocols so that I can determine whether we have the necessary resources to undertake the trial. It can be hard work, and for me to be effective I have to have a good understanding of how each of our trusts’ imaging modalities function. I also need to have strong communication skills, especially in regards to explaining radiography perspectives to multi-disciplinary team members who may have little to no understanding of imaging. More than this, I need to be able to form and maintain good relations with all sides to ensure that effective communication can take place.
The work I do allows for better outcomes between radiology and research departments. It also affords me the opportunity to be a part of progress, seeking out better practice or improved technology for the future of imaging. In addition, I am able to undertake my own research, working towards my goals of further academic qualifications.
My role is important. I feel that I and my work contributions are valued by both the radiology and research teams. My pathway for personal development is clear and I am able to see the benefits in the set-up and management of the trials my Trust undertakes.
What is Radiography research and why is it important?
There is often research aimed at improving and advancing the field of diagnostic imaging. Currently there are trials into new scanning techniques; new equipment with the potentials for dose reduction and/or improved image quality and patient experiences; and the use of AI in imaging and reporting.
The benefits of improvements in our field are numerous. Every radiographer wants to give patients the best experience they can, however this is often at odds with the nature of our job. Requiring patients to hold uncomfortable positions when they are in pain or worried; perhaps having to go through narrow tubes which are sometimes incredibly loud; needing injections which makes them feel weird or mean they are radioactive and have to keep distance from other people at a time when they could really do with support. With research, we can aim to improve these experiences; reduce scan times or radiation exposures, wider bore scanners or open scanners, even finding new imaging or testing which removes the need for the ionising radiation all together!
Patients are at the heart of the NHS, and diagnostic imaging is often an area in which a good patient experience can be harder to provide (that is not to say that we don’t try!). With research, we have the potential to make those improvements to service, to provide for our patients in the way which we want to and the way that they deserve.
How can I get involved?
Often, radiography research is overseen by radiologists, doctors and orthopaedic surgeons, but there is no reason why radiographers shouldn’t also get involved. As we are the ones who use the equipment on a daily basis, consent and care for the patients during imaging, and come into contact with the faults and issues. Our profession contains a wealth of knowledge which can be used to improve all aspects of radiography.
You don’t need any academic qualifications to get started with research activities. In fact, many radiographers image research patients without being privy to the research aims. In a busy department, such patients are treated the same as any other in most regards. If you do image a research patient, perhaps look into the trial itself. As well as being interesting additional information, it can be used as material for CPD in the form of a case study or reflective piece. You may also discover potential ways to improve the patient experience within your department and help to enact future change.
Look into what your hospital requires for research involvement. The Good Clinical Practice (GCP) qualification, which is usually necessary, can be found for free as an online e-learning module. The NIHR website provides a lot of helpful information for getting started. NIHR also provides help for those who are wanting to gain further academic qualifications, such as through grant applications for fellowship awards. These are highly competitive but allow better access for NHS employees to undertake Masters or Doctorate level qualifications. The NIHR also run conferences for those who are new to research but interested in how they can take part.
You could also look at taking part in your department’s audits. Audits are a great way to check in on the health of your department, what you are doing well, and what you can improve on. Audit skills can also overlap with those necessary for research work, as well as provide possible avenues for research within your department.
How do I get a research job?
The roles of radiographers in research are expanding. Some hospitals offer clinical research radiographer positions, which give additional responsibility to train for and undertake specialised research imaging, often alongside a multi-disciplinary team. Other trusts may offer training for those wanting to aid research trials.
For research-specific roles, take a look at NHS jobs. You will find posts for Research Radiographers or Research Clinical Practitioners/AHPs. When I applied for my Audit and Research radiographer post, I had no specific research skills however I was well versed in audits and had learned about the processes of research in my own time. Enthusiasm goes a long way when applying for research roles, we need radiographers who are driven and raring to get stuck in.
There is so much experience and knowledge that radiographers have to offer research, and there’s so much improvement and advancement to be received in turn. I strongly encourage any radiographers to give it a try. You never know, you may get hooked!
To submit your research to a BIR journal find out more here:
Kim Mason is a HCPC registered diagnostic radiographer, graduating from the University of Leeds with a 1st Class BSc Honours in Diagnostic Radiography in 2018. They have experiences in education both inside and outside of radiography, and have a passion for improving the radiography services in the UK.
Kim has multiple chronic conditions, and as such, they are an ambulatory wheelchair user. This has given them keen insight into the experiences of patients within the radiography department, having undergone imaging in most modalities as a patient. They have a vested interest in educating the public about radiography, and educating radiographers on improvements to patient care.
Radiation oncology clinics face numerous challenges in the present environment, including the simultaneous management of multiple tasks (many of which are manual in nature), various degrees of standardisation, and the potential for errors to impact patient treatment. Automation can help address these challenges by reducing the time required to execute manual portions of the workflow and positively impacting the quality and safety of patient care. Tyler Blackwell, Medical Physicist discusses more:
Efficiency
To a large degree, many departments have already integrated automation into their departments. However, it stands to be a driving force of innovation in our field for the foreseeable future, coinciding with efforts to improve plan quality and reduce errors inherent in human interaction. Increasing the productivity and efficiency of our daily clinical tasks by minimizing time spent on tedious, routine tasks “below our licenses” (as worded by physicist Eric Ford as part of a Radformation Focal Spot interview) allows more time to address other critical clinical elements that require human expertise.
In developing smarter tools, we have an opportunity to improve the patient experience. Radformation CEO Kurt Sysock, MS, DABR, explains, “On average, it takes five days after simulation to create a finished plan that is ready for treatment, and we want to reduce that to less than one day.” Indeed, reducing the time between simulation and treatment can have a significant impact not only on patient satisfaction, but also on patient outcomes. Delays in treatment planning times are associated with an overall higher risk of mortality ranging from 1.2–3.2% per week for curative diseases. Reducing the time between simulation and treatment maximizes tumor control probability and patient survival.
Quality and Safety
The quality and consistency of patient care are greatly improved when the care team is able to deliver treatment as efficiently as possible. In this environment, they can devote more resources toward tasks that require greater attention or collective experience. From the clinician’s point of view, smart automation reduces the time spent on tasks that do not add value to patient care but are nonetheless important for sustaining operations.
Over the last decade, clinicians have largely embraced a culture of safety and quality improvement. This paradigm shift delivers a number of benefits for patients and involves a continued effort toward reducing errors in radiation oncology. While a number of interventions can positively influence safety and quality, automation is highly effective in this regard. Absent automation, this ongoing commitment will be inhibited by a lack of efficiency and scalability as clinicians grapple with manual processes and endless checklists.
Automation is one of the most effective ways to impact change in medicine. Source: Cafazzo, J and St-Cry, O. From Discovery to Design: The Evolution of Human Factors in HealthCare. Healthcare Quarterly. April 2012. doi:10.12927/hcq.2012.22845
Automation plays a part in advances in clinical care as well. Radformation CSO Alan Nelson, DMP, DABR, argues that, “just as IMRT significantly improved the effectiveness of treatment while reducing side-effects, automation will enable the field to explore and implement new solutions for therapy protocols that otherwise simply would not have been feasible due to lack of resources.”
An Elevated Workflow At Every Step
Finding steps along the treatment care path that involve manual inputs isn’t a challenge. Wherever they exist, there is an opportunity for automation to provide value. From planning and on-treatment to billing and quality assurance, the results of these workflow improvements are impressive.
Structure Segmentation
The proper delineation of anatomical structures in the vicinity of the target is important in understanding the impact of a treatment plan on the surrounding healthy tissues. But manual contouring can be resource-intensive, and some structure boundaries—especially for target structures—can vary widely based on who is performing the work. According to physicist Noah Bice of New York University Langone, “Contouring is subjective. With any mix of individuals, there are inherently varying levels of expertise and personal preference involved.”
Within the past few years, the introduction of deep-learning algorithms for contouring has transformed the landscape. By exploiting cloud-based computational resources, structure sets, including organs-at-risk and target structures, can be generated in a fraction of the time as manual contours. Departments have been quick to adopt this new technology, which will likely become a global standard of care within the decade.
Treatment Planning
Given that every patient’s anatomy and disease state is unique, it might feel safe to assume that it may not be possible to automate this process. Despite this inherent variation, the approach to planning is algorithmic and repetitive. By scripting various repetitive processes—field-in-field or electronic compensator planning, for example—departments are capable of producing consistently high-performing plans in a fraction of the time.
This process, when applied to the Halcyon machine, has made it feasible to plan electronic compensator breast plans when otherwise manual planning is impractically cumbersome and time-consuming.
Plan Evaluation and Reporting
Determining the quality of any given treatment plan is no small task. Often, it is not easy to compare comprehensive plan quality elements within the treatment planning system (TPS). By tapping into the plan data via scripting interfaces, it’s possible to pull dosimetric information for comparison against dose constraint templates to verify the quality of a plan during or after the plan is complete.
Automated platforms are quickly becoming the standard of care, providing intuitive assessments of plan quality, including dose constraints, plan checks, machine collision risk, and reporting. While default TPS reports are often limited in scope, third-party options offer fast, customized plan reports as well as the ability to populate directly into ARIA Documents.
Comprehensive new tools allow for faster, user-friendly plan revaluation and reporting.
Quality Assurance
Collecting and sorting quality assurance information can be a challenging task given the variety of equipment and vendor products in the clinic that requires tracking. The frequency of the tasks adds another layer of complexity as well, with new data being acquired daily. Thankfully, new quality assurance platforms make short work of managing this data, providing a central location for all data from linacs and CTs to ionisation chambers and GM meters. Automation is capable of detecting new test information—from daily or monthly tests—and effortlessly syncing data to the centralized platform for quick analysis and review. These databases bring efficiency while reducing the dependency on multiple separate spreadsheets in unique locations.
Conclusion
In conclusion, the use of intelligent automation in radiation oncology—such as the solutions offered by Radformation—has the potential to revolutionize clinical workflows, leading to bottom-line improvements in patient care. By reducing the time required to execute manual portions of the workflow, clinicians can devote more time to critical clinical elements that require human expertise, such as addressing treatment planning and ensuring patient safety. Automation also plays a part in advances in clinical care and enables the field to explore and implement new solutions that may not have been feasible without this technology. In short, the benefits of automation in radiation oncology are numerous and diverse, and they can significantly enhance the overall quality and safety of patient care.
Tyler Blackwell, MS, DABR, is a medical physicist at Radformation focused on clinical collaborations and community engagement. Before joining Radformation, he spent a decade working as a clinical physicist. He is active on several committees for the American Association of Physicists in Medicine, including the board of directors, and volunteers for the American Board of Radiology.





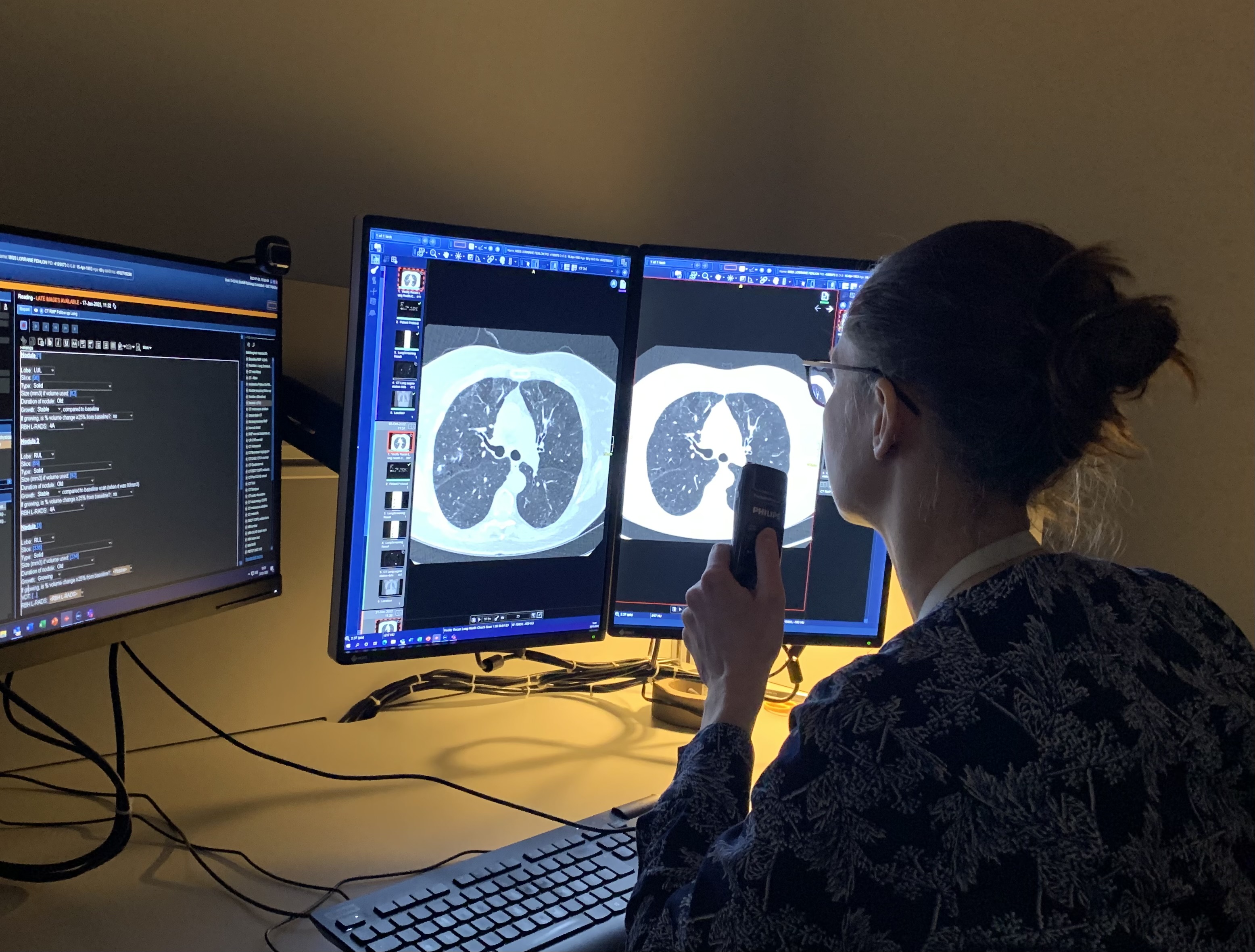


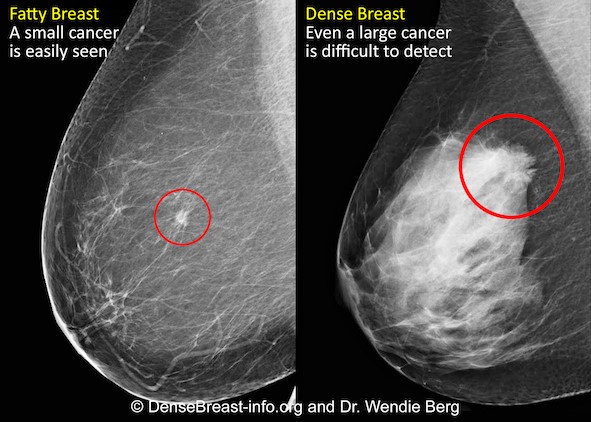
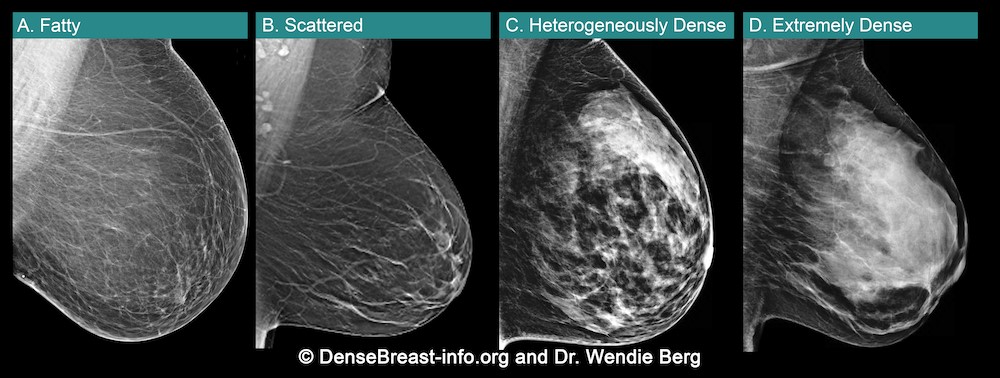
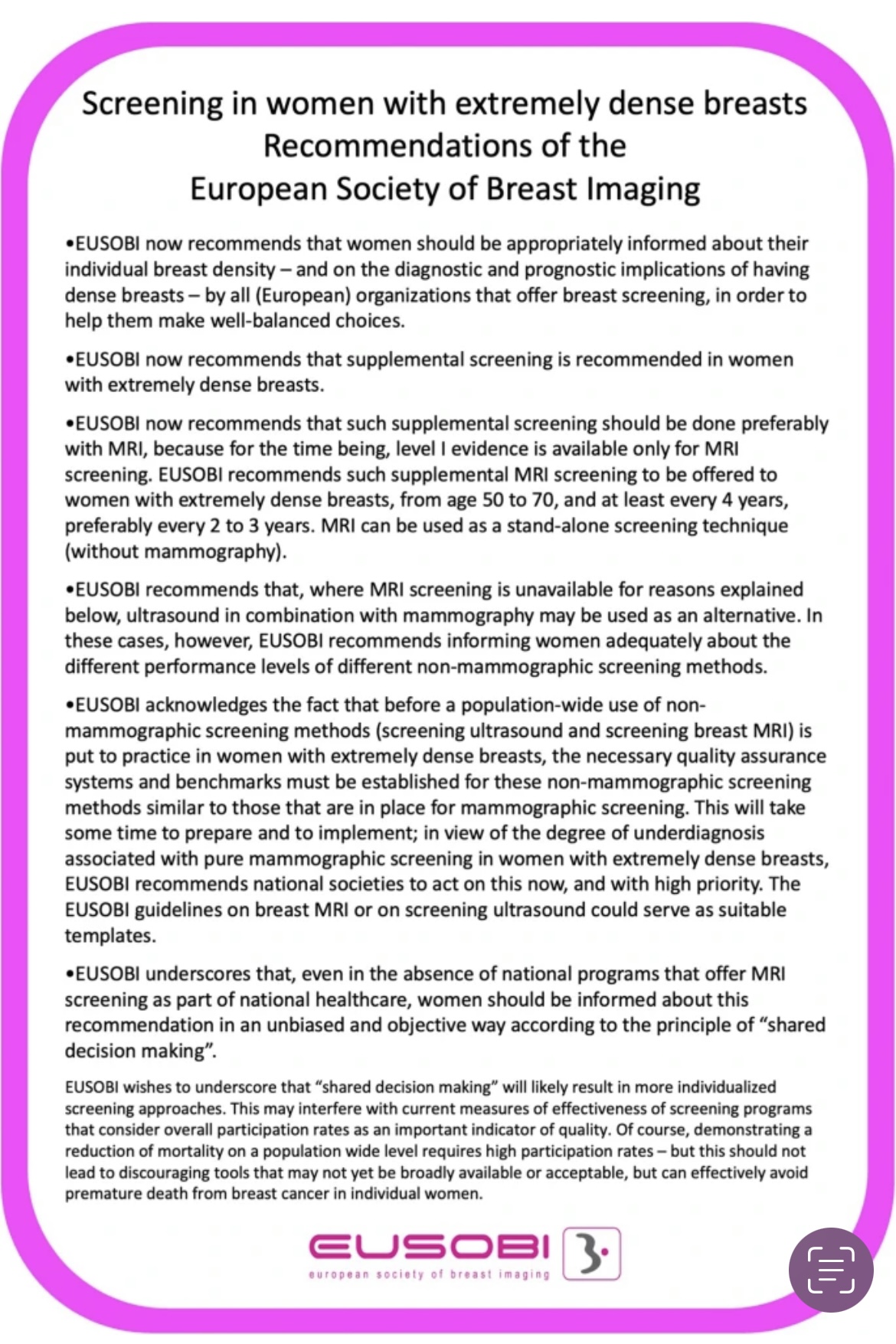


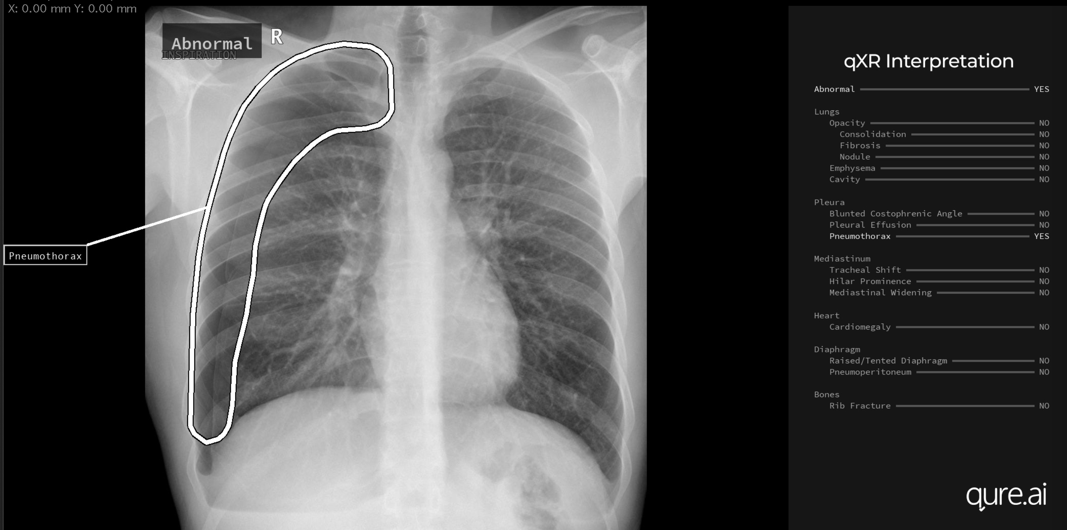

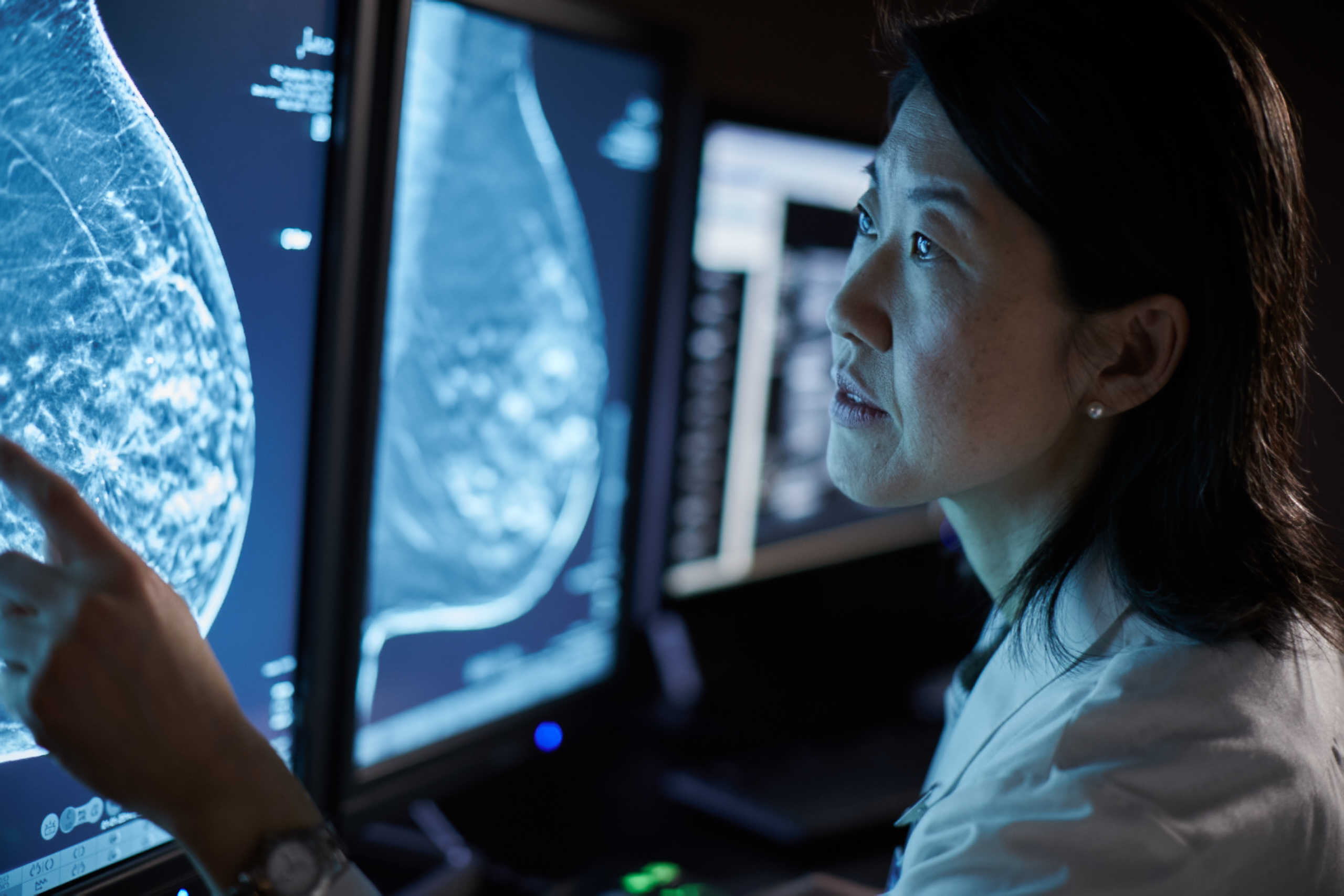





























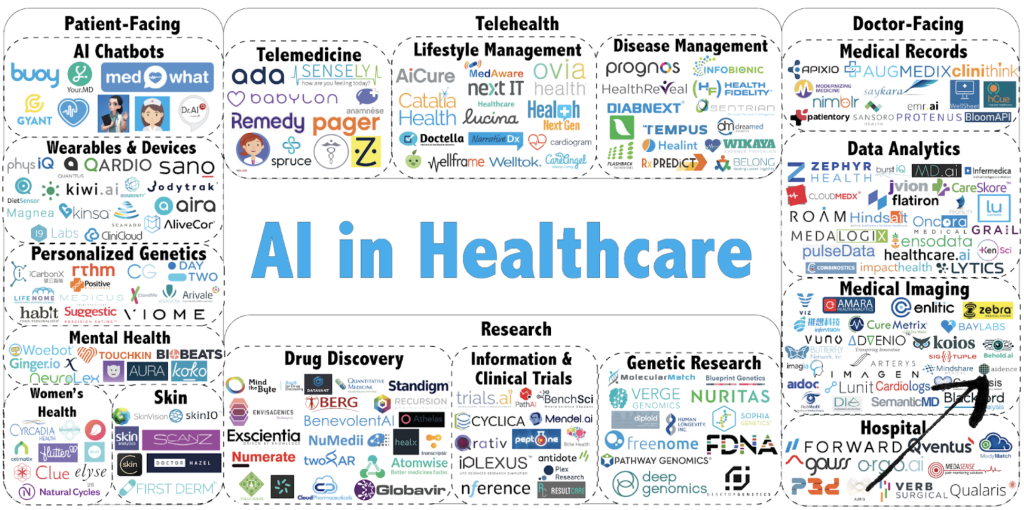

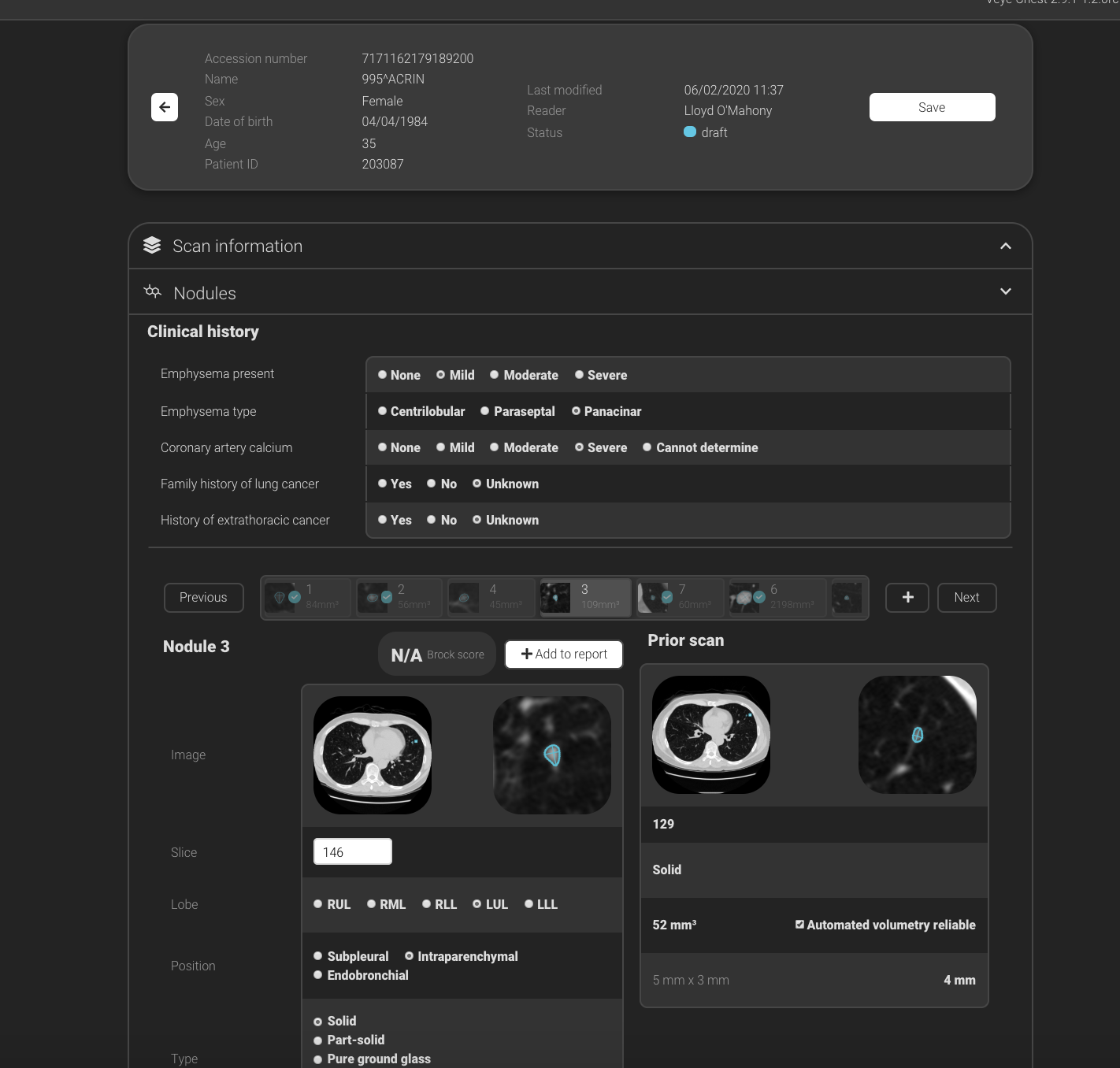


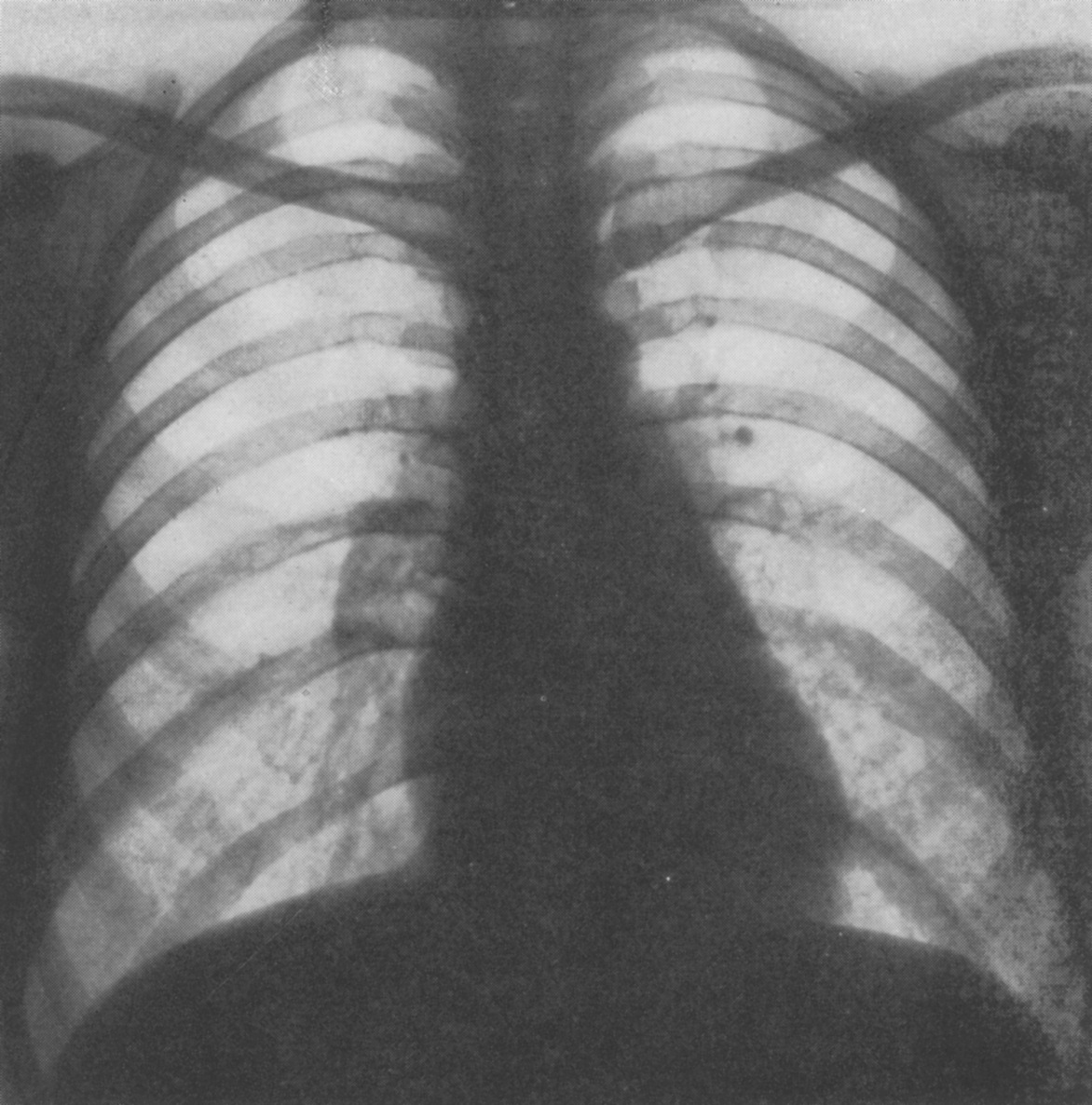

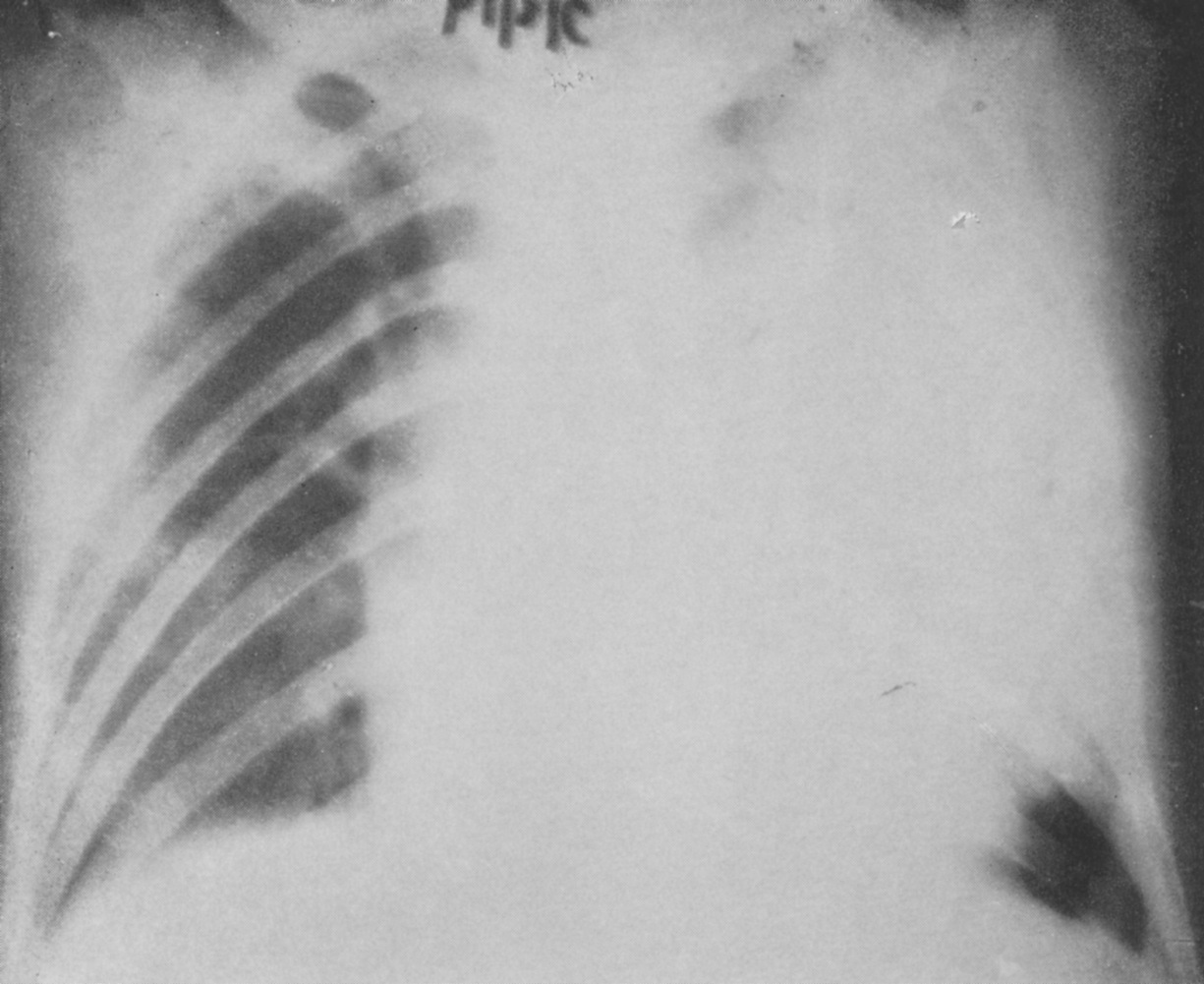
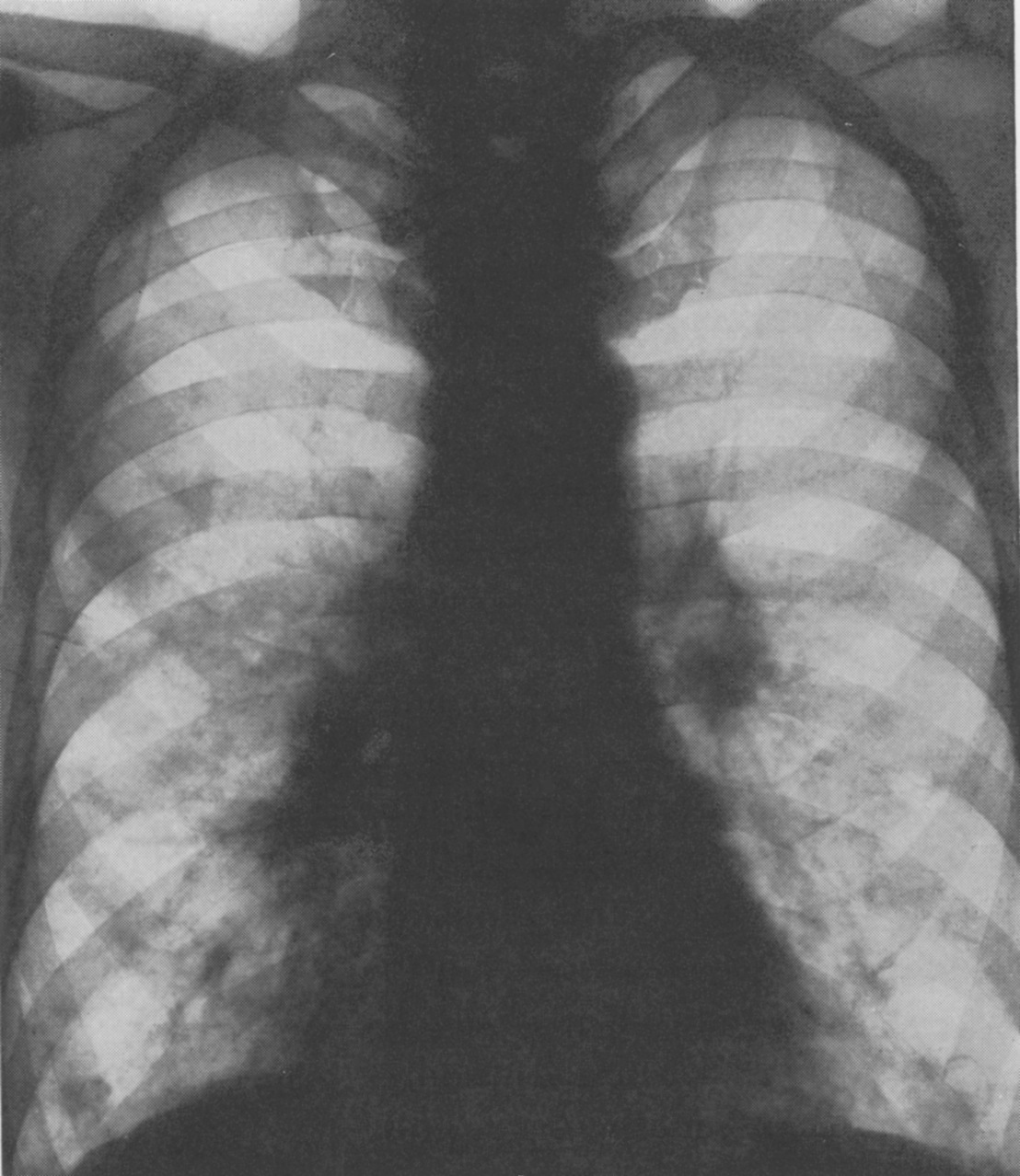
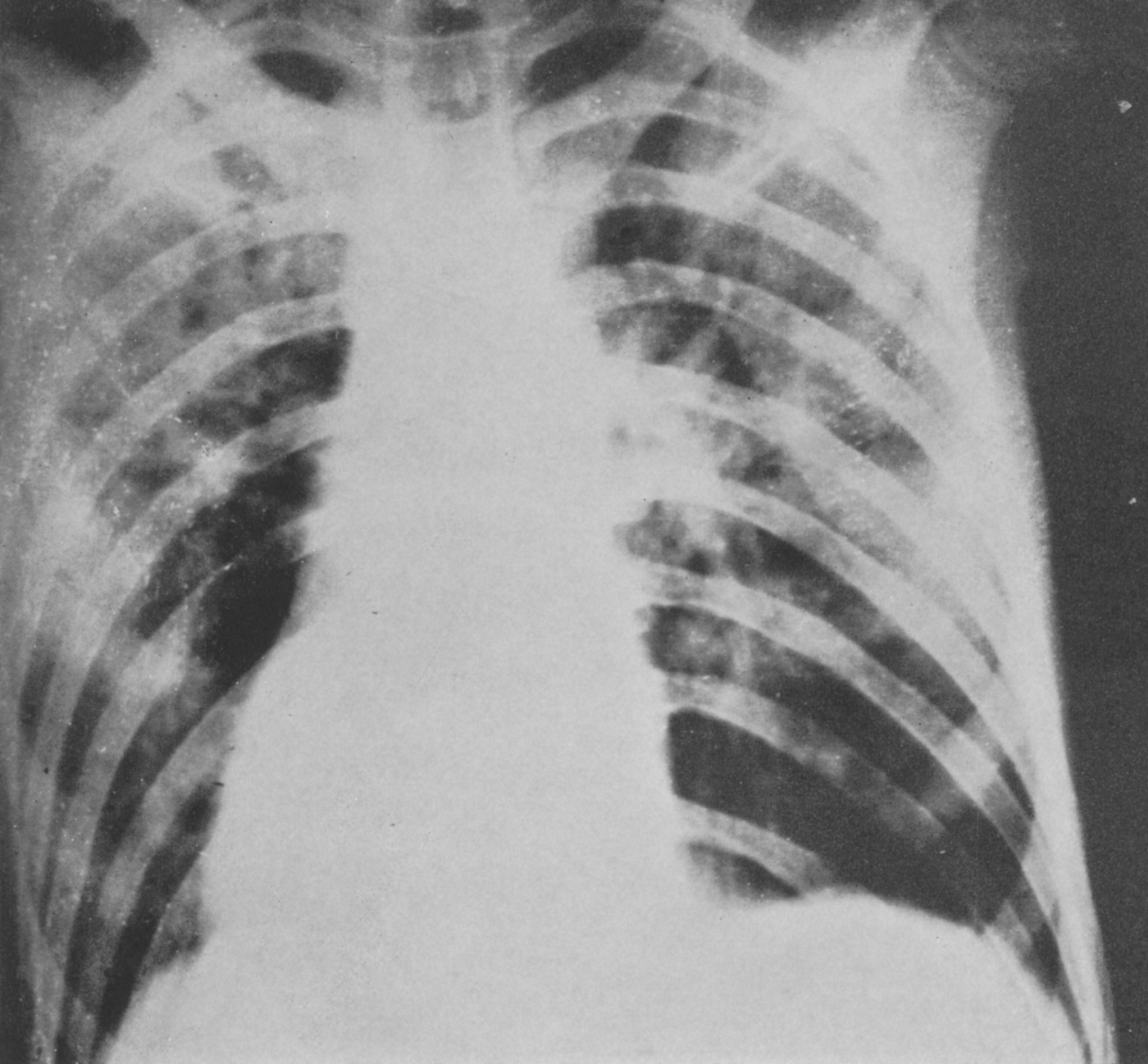

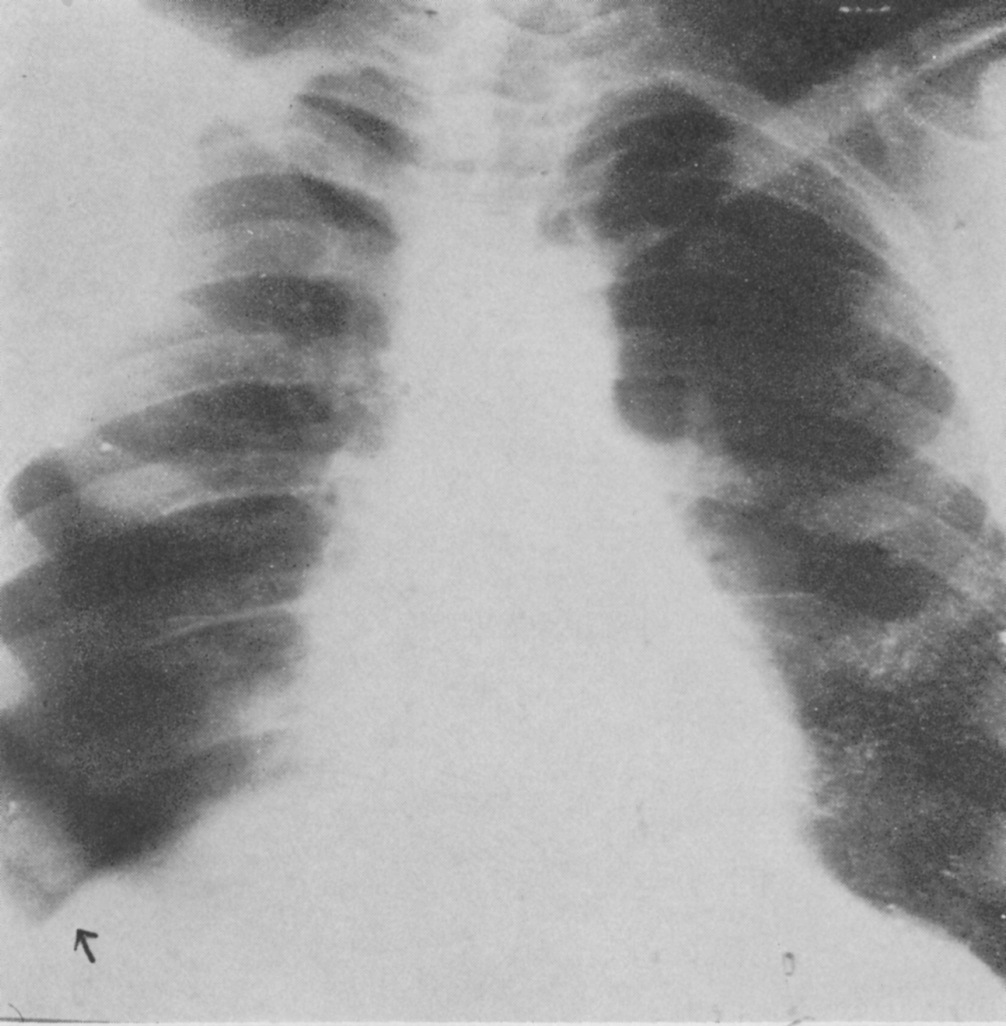
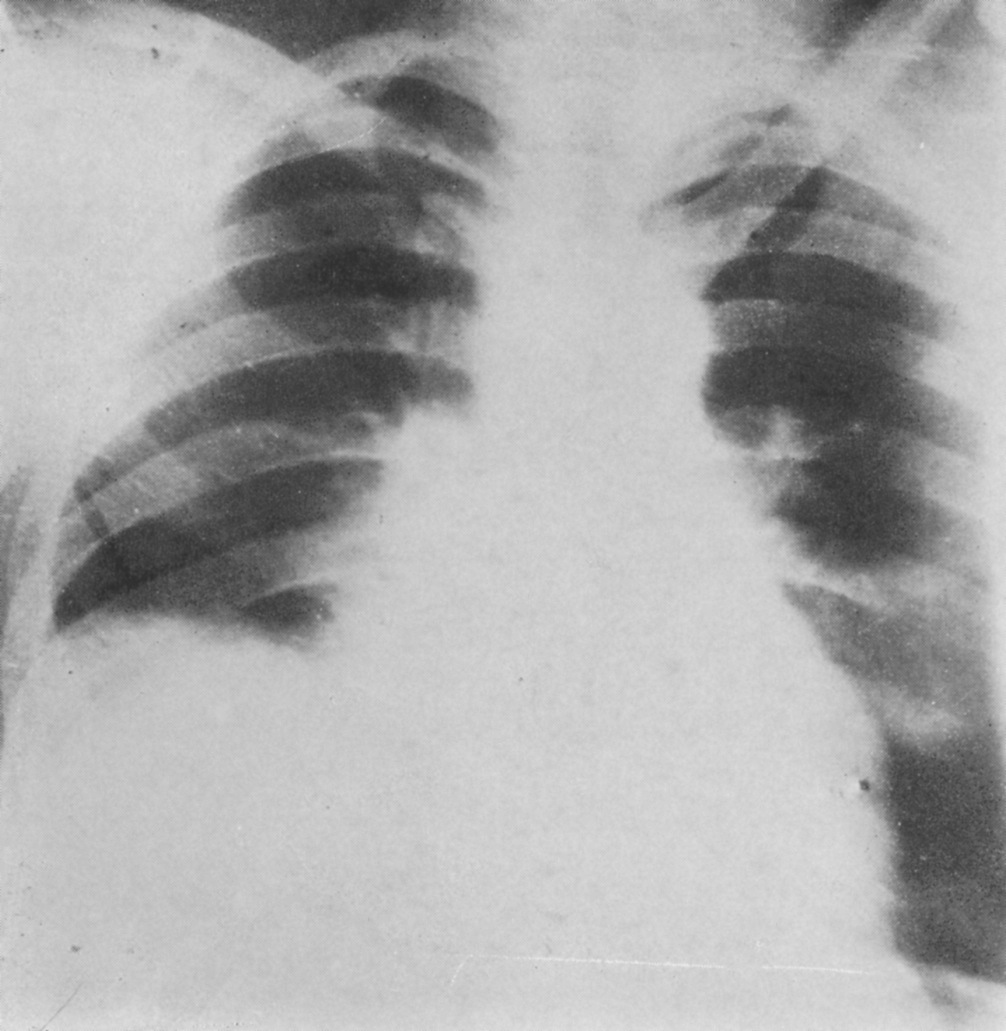


 My week was spread between plain film, ultrasound, CT, MRI and some interventional radiology sessions. While the plain film sessions were useful to carry into my regular job, the IR experience in the theatre was quite thrilling. Interventional radiologists are clinicians with those magic wands (catheters) who practice some seemingly futuristic medicine. It was an absolutely inspiring experience for me.
My week was spread between plain film, ultrasound, CT, MRI and some interventional radiology sessions. While the plain film sessions were useful to carry into my regular job, the IR experience in the theatre was quite thrilling. Interventional radiologists are clinicians with those magic wands (catheters) who practice some seemingly futuristic medicine. It was an absolutely inspiring experience for me. Radiologists are happy people: Having rotated through various departments during my internship and experiencing a few departments in the NHS, I found a striking difference in how radiologists see their work. They work as a team, care for each other and are very encouraging. Don’t be surprised if your fellow consultant is making you a cup of coffee! Also, the trainees fairly support medical students and junior doctors in walking the path to enter specialty training. Overall, I felt that the happiness index of radiologists was higher than other specialists and they truly enjoy their work.
Radiologists are happy people: Having rotated through various departments during my internship and experiencing a few departments in the NHS, I found a striking difference in how radiologists see their work. They work as a team, care for each other and are very encouraging. Don’t be surprised if your fellow consultant is making you a cup of coffee! Also, the trainees fairly support medical students and junior doctors in walking the path to enter specialty training. Overall, I felt that the happiness index of radiologists was higher than other specialists and they truly enjoy their work.
 This was a time when, in this Cinderella of specialties, physics planning was achieved by the superposition of two dimensional radiation plots (isodoses) ,using tracing paper and pencils, to produce summated maps of the distribution. The crude patient outlines were derived from laborious isocentric distance measurements augmented by the essential “flexicurve”. The whole planning process was slow and labour intensive fraught with errors and ridiculed by colleagues in the perceived prestigious scientific and clinical disciplines. The principal platform for external beam radiotherapy delivery, the Linear Accelerator (LinAc), had also reached something of a plateau of development, albeit with improved reliability, but few fundamental changes. Caesium tubes were transported from the “radium safe”, locked in an underground vault, to the operating theatre in a lead-lined trolley, where they were only loaded into “central tubes” and “ovoids” after the examination under anaesthetic (which was performed with the patient in the knee-chest position); they were then manually placed into the patient, who went to be nursed on an open ward, albeit behind strategically placed lead barriers.
This was a time when, in this Cinderella of specialties, physics planning was achieved by the superposition of two dimensional radiation plots (isodoses) ,using tracing paper and pencils, to produce summated maps of the distribution. The crude patient outlines were derived from laborious isocentric distance measurements augmented by the essential “flexicurve”. The whole planning process was slow and labour intensive fraught with errors and ridiculed by colleagues in the perceived prestigious scientific and clinical disciplines. The principal platform for external beam radiotherapy delivery, the Linear Accelerator (LinAc), had also reached something of a plateau of development, albeit with improved reliability, but few fundamental changes. Caesium tubes were transported from the “radium safe”, locked in an underground vault, to the operating theatre in a lead-lined trolley, where they were only loaded into “central tubes” and “ovoids” after the examination under anaesthetic (which was performed with the patient in the knee-chest position); they were then manually placed into the patient, who went to be nursed on an open ward, albeit behind strategically placed lead barriers. In the latter half of the eighties these solutions began to crystallise. Computers were being introduced across the NHS and their impact was not lost in radiotherapy. Pads of tracing paper were replaced with the first generation of planning computers. The simple “Bentley-Milan” algorithms could account for patient outlines accurately and speedily and optimising different beam configurations became practical. Consideration of Organs at Risk, as defined by the various International Commission on Radiation Units (ICRU) publications, became increasingly relevant. Recognition of the importance of delineating the target volumes and protecting normal tissue required improved imaging and this was provided by the new generation of CT scanners. In the nineties these were shared facilities with diagnostic radiology departments. However, the improvements provided by this imaging, enabling accurate 3-dimensional mapping of the disease with adjacent normal tissues and organs at risk, dictated their inclusion into every radiotherapy department soon after the millennium. The added bonus of using the grey scale pixel information, or Hounsfield numbers, to calculate accurate radiation transport distributions soon followed when the mathematical and computer technology caught up with the task. The value of MR and Positron Emission Tomography (PET) imaging was also recognised in the diagnosis, staging and planning of radiotherapy and the new century saw all of these new technologies embedded within the department.
In the latter half of the eighties these solutions began to crystallise. Computers were being introduced across the NHS and their impact was not lost in radiotherapy. Pads of tracing paper were replaced with the first generation of planning computers. The simple “Bentley-Milan” algorithms could account for patient outlines accurately and speedily and optimising different beam configurations became practical. Consideration of Organs at Risk, as defined by the various International Commission on Radiation Units (ICRU) publications, became increasingly relevant. Recognition of the importance of delineating the target volumes and protecting normal tissue required improved imaging and this was provided by the new generation of CT scanners. In the nineties these were shared facilities with diagnostic radiology departments. However, the improvements provided by this imaging, enabling accurate 3-dimensional mapping of the disease with adjacent normal tissues and organs at risk, dictated their inclusion into every radiotherapy department soon after the millennium. The added bonus of using the grey scale pixel information, or Hounsfield numbers, to calculate accurate radiation transport distributions soon followed when the mathematical and computer technology caught up with the task. The value of MR and Positron Emission Tomography (PET) imaging was also recognised in the diagnosis, staging and planning of radiotherapy and the new century saw all of these new technologies embedded within the department. LinAc technology also received added impetus. Computers were firstly coupled as a front end to conventional LinAcs as a safety interface to reduce the potential for “pilot error”. Their values were soon recognised by the manufacturers and were increasingly integrated into the machine, monitoring performance digitally and driving the new developments of Multi Leaf Collimators (MLC) and On Board Imaging (OBI).
LinAc technology also received added impetus. Computers were firstly coupled as a front end to conventional LinAcs as a safety interface to reduce the potential for “pilot error”. Their values were soon recognised by the manufacturers and were increasingly integrated into the machine, monitoring performance digitally and driving the new developments of Multi Leaf Collimators (MLC) and On Board Imaging (OBI). Dr David A L Morgan began training in Radiotherapy & Oncology as a Registrar in 1977, and in 1982 was appointed a Consultant in the specialty in Nottingham, continuing to work there until his retirement in 2011. He joined the BIR in 1980 and at times served as Chair of its Oncology Committee and a Member of Council. He was elected Fellow of the BIR in 2007. He is author or co-author of over 100 peer-reviewed papers on various aspects of Oncology and Radiobiology.
Dr David A L Morgan began training in Radiotherapy & Oncology as a Registrar in 1977, and in 1982 was appointed a Consultant in the specialty in Nottingham, continuing to work there until his retirement in 2011. He joined the BIR in 1980 and at times served as Chair of its Oncology Committee and a Member of Council. He was elected Fellow of the BIR in 2007. He is author or co-author of over 100 peer-reviewed papers on various aspects of Oncology and Radiobiology. Andy Moloney completed his degree in Physics at Nottingham University in 1980 before joining the Medical Physics department at the Queens Medical Centre in the same city. After one year’s basic training in evoked potentials and nuclear medicine, he moved to the General Hospital in Nottingham to pursue a career in Radiotherapy Physics and achieved qualification in 1985. Subsequently, Andy moved to the new radiotherapy department at the City Hospital, Nottingham, where he progressed up the career ladder until his promotion as the new head of Radiotherapy Physics at the North Staffordshire Royal Infirmary in Stoke-on-Trent. Over the next twenty years Andy has acted as Clinical Director for the oncology department and served on the Radiation Physics and Oncology Committees at the BIR and was appointed a Fellow in 2007. He has been the author and co-author of multiple peer reviewed articles over the years prior to his retirement in 2017.
Andy Moloney completed his degree in Physics at Nottingham University in 1980 before joining the Medical Physics department at the Queens Medical Centre in the same city. After one year’s basic training in evoked potentials and nuclear medicine, he moved to the General Hospital in Nottingham to pursue a career in Radiotherapy Physics and achieved qualification in 1985. Subsequently, Andy moved to the new radiotherapy department at the City Hospital, Nottingham, where he progressed up the career ladder until his promotion as the new head of Radiotherapy Physics at the North Staffordshire Royal Infirmary in Stoke-on-Trent. Over the next twenty years Andy has acted as Clinical Director for the oncology department and served on the Radiation Physics and Oncology Committees at the BIR and was appointed a Fellow in 2007. He has been the author and co-author of multiple peer reviewed articles over the years prior to his retirement in 2017.